Your teeth provide a detailed account of your life, much as a tree's rings record its history, a groundbreaking study shows.
"A tooth is not a static and dead portion of the skeleton. It continuously adjusts and responds to physiological processes," said lead study author Paola Cerrito, a doctoral candidate studying anthropology and dentistry at New York University (NYU) in New York City.
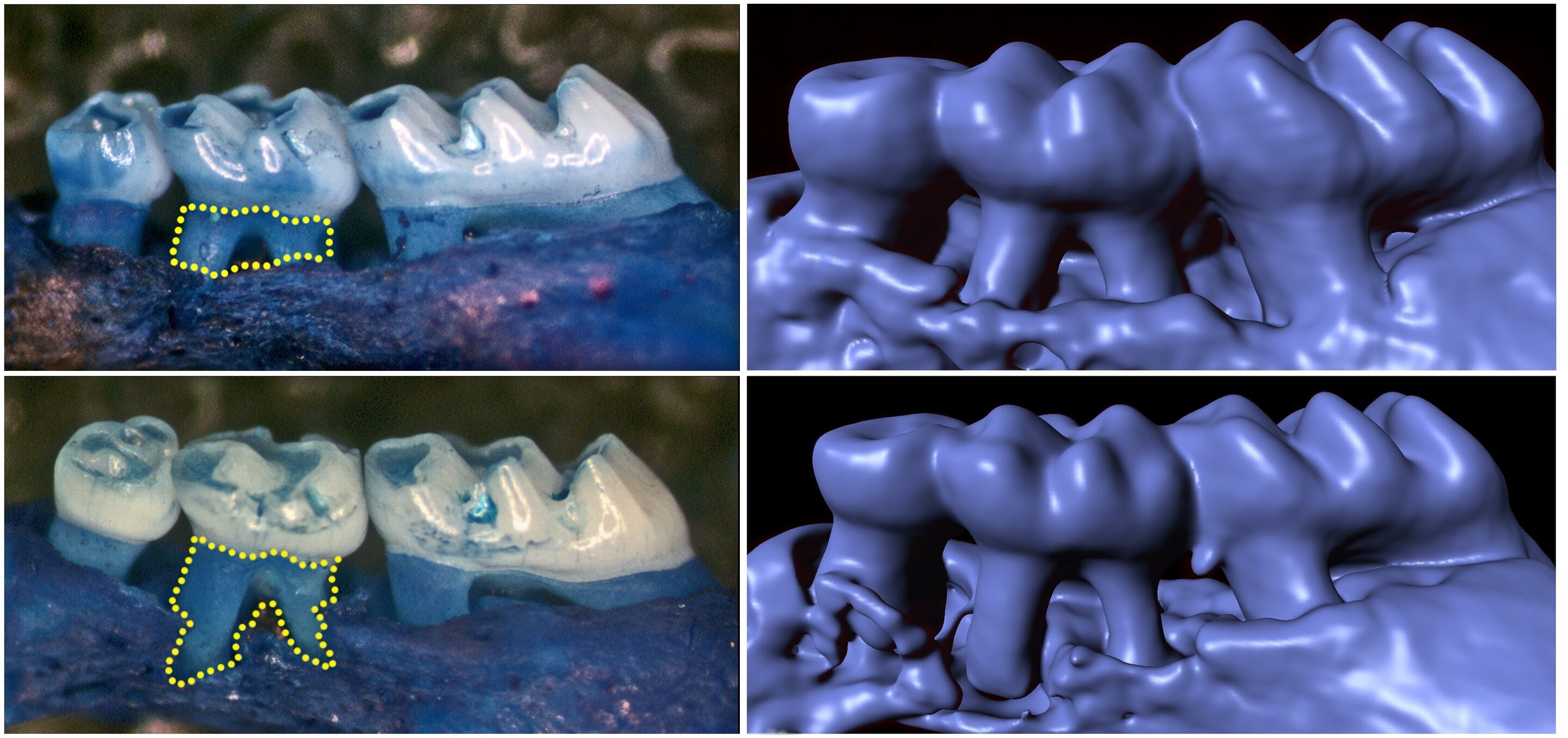
"Just like tree rings, we can look at 'tooth rings': continuously growing layers of tissue on the dental root surface," she said in a university news release. "These rings are a faithful archive of an individual's physiological experiences and stressors from pregnancies and illnesses to incarcerations and menopause that all leave a distinctive permanent mark."
For the study, the NYU researchers compared nearly 50 teeth from skeletons of people who ranged in age from 25 to 69 to information about their medical history and lifestyle, such as age, illnesses, significant events and where they lived.
The researchers focused on cementum, the tissue covering the tooth's root. It begins to form yearly layers from the time the tooth appears in the mouth.
Using imaging techniques to illuminate cementum bands, the investigators uncovered links between tooth formation and various events in the lives of those included in the study.
"The cementum's microstructure, visible only through microscopic examination, can reveal the underlying organization of the fibers and particles that make up the material of this part of the tooth," Cerrito said.
According to study co-author Timothy Bromage, a professor at NYU's College of Dentistry, "The discovery that intimate details of a person's life are recorded in this little-studied tissue promises to bring cementum straight into the center of many current debates concerning the evolution of human life history."
Periodontitis is a serious gum disorder induced by an imbalance in the bacteria and other microorganisms of the mouth (the oral microbiome). It is the sixth-most prevalent infectious disease and the most common cause of tooth loss worldwide.
Monell Center Director and President Robert Margolskee, MD, PhD and cell biologist Marco Tizzano, PhD, along with colleagues from Sichuan University, found that the newly identified cells, known as solitary chemosensory cells (SCCs), are present in the gums of mice. Here they express several types of taste receptors along with a downstream coupling protein called gustducin. SCCs are taste-like chemical detectors that sense irritants and bacteria, and biologists have found them throughout the gut, urinary tract, nasal cavities, and now in the gums.
"These sensory cells may provide a new approach for personalized treatment of periodontitis by harnessing a person's own innate immune system to regulate their oral microbiome," said Margolskee.
The team showed that knocking out taste-signaling molecules like gustducin or genetically removing gum SCCs in the mice leads to overgrowth of pathogenic oral bacteria and periodontitis. Conversely, stimulating bitter taste receptors in SCCs promotes the production of anti-microbial molecules.
Mice without gustducin in their SSCs have a more damaging set of microbes living in their mouths compared to normal mice, implying that the lack of gustducin disconnects the sentinel cells' molecular signal to other systems. Importantly, differences in the oral bacterial composition of the gustducin-less mice compared to normal mice occurred before any loss of bone in the gums, implying that differences in the oral microbiome could be used as a harbinger of disease.
In previous studies with other tissues, researchers found that activating the bitter taste receptor TAS2R38, which is expressed in human nasal SCCs, stimulates the secretion of antimicrobial peptides (AMPs) that repress the growth of respiratory pathogens. To examine the effects of repeated stimulation of gum SCCs on periodontitis (and the release of gum AMPs) in the current study, the researchers applied a mouthwash containing the ultra-bitter substance denatonium to the gums of the mice twice a day. This activated gum SCCs as well as their antimicrobial molecules, which reduced periodontitis in normal mice, but not in the periodontitis-susceptible animals without gustducin.
After receiving the denatonium, normal mice showed an enhanced release of an AMP called β-defensin, which was produced at more than twice the levels seen in control mice treated only with saline mouthwash. On the other hand, when the gustducin-less mice were given denatonium mouthwash, there was no effect on the level of β-defensin.
"Our study adds to a growing list of tissues we now know contain SCCs and indicates that the common molecular pathways in gum SCCs are involved in the regulation of oral microbiota," said Tizzano. "In the absence of taste signaling in the gums, the oral microbiome changed in mice without gustducin."
From this animal study, and unpublished work in humans, the team expects that gum SCCs in humans play a similar role in regulating the make-up of the oral microbiome, notes coauthor Xin Zheng, a dental science researcher from the National Clinical Research Center for Oral Diseases, West China Hospital of Stomatology. They surmise that since genetic differences in taste receptors are commonly detected in people, particularly loss-of-function of the bitter taste receptor TAS2R38, the dysfunction of taste-receptor-mediated innate immune responses could be used for dental chair-side screening for individuals who may be most susceptible to oral infectious diseases.
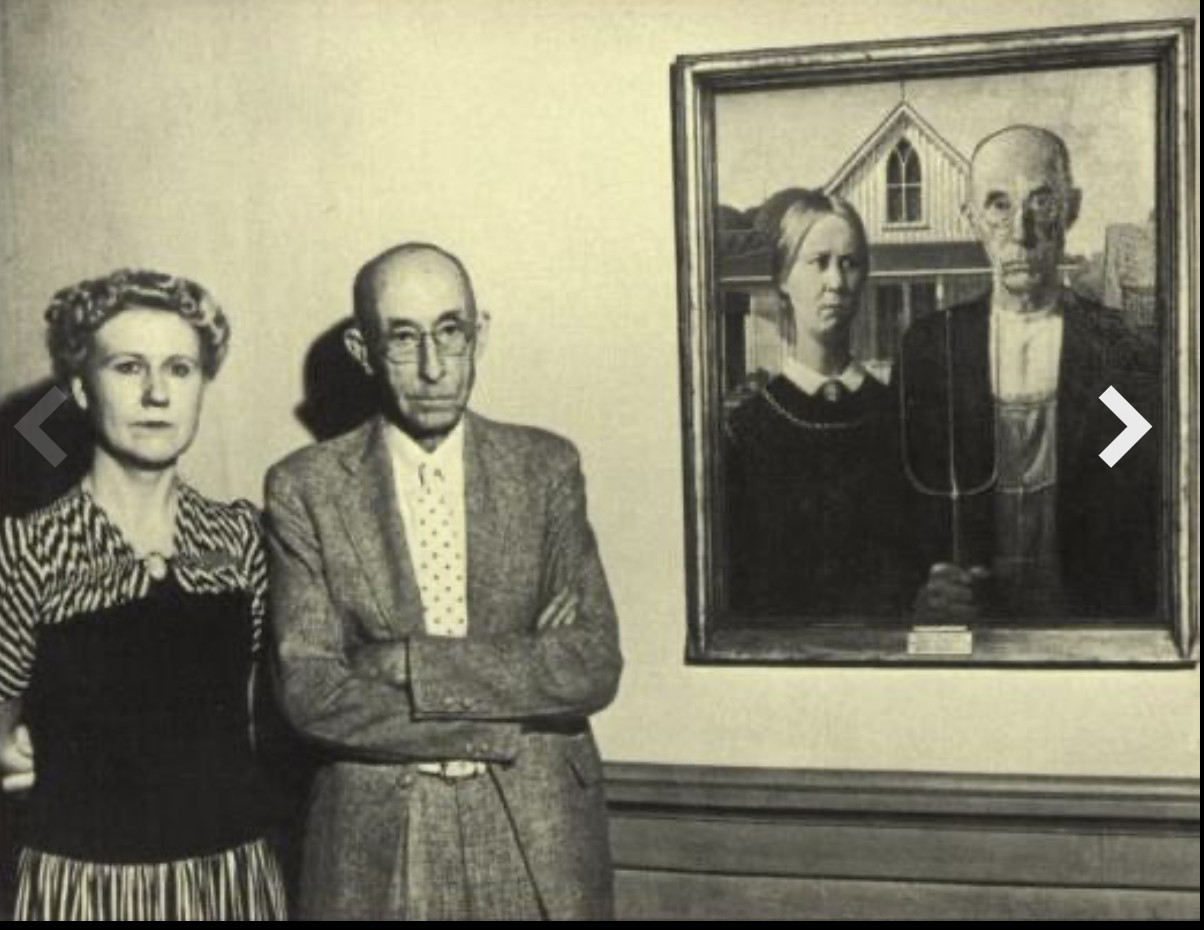
Dr Byron McKeeby agreed to model for his friend. Grant Wood painted him in his dental office in the Cedar Rapids Savings Bank Building (now the Guaranty Bank Building). McKeeby was 62. He donned overalls and held a theater prop pitchfork. The rest of the painting, including the farm woman, which his sister, Nan, posed for, was executed a few blocks away in his studio loft at No. 5 Turner Alley.
Grant Wood said he’d exaggerate McKeeby’s features so no one would recognize him.
McKeeby distanced himself from the painting as it took the country by storm. Friends thought it was him and even joked about the pitchfork’s role in his dental procedures, but McKeeby stood firm in his denials.
He was known for his dapper style and affable sense of humor. The real McKeeby was nothing like the dour farmer who challenged the painting’s viewers.
It was literally national news when McKeeby broke his silence in 1935 and admitted that, yes, he was the farmer with the pitchfork.
As the model for the solemn farmer in Grant Wood's iconic painting, Dr B H Mc Keeby is one of the famous figures in modern portrait art although his name is little known.
He studied dentistry at the University of Iowa, graduating in 1894 and founding his first practice in Winthrop, IA. He moved to Cedar Rapids in 1901 where he established an office which he maintained almost until his death. It was here that Grant Wood, who was one of McKeeby's patients, approached him to model as the father of the farmer's daughter.
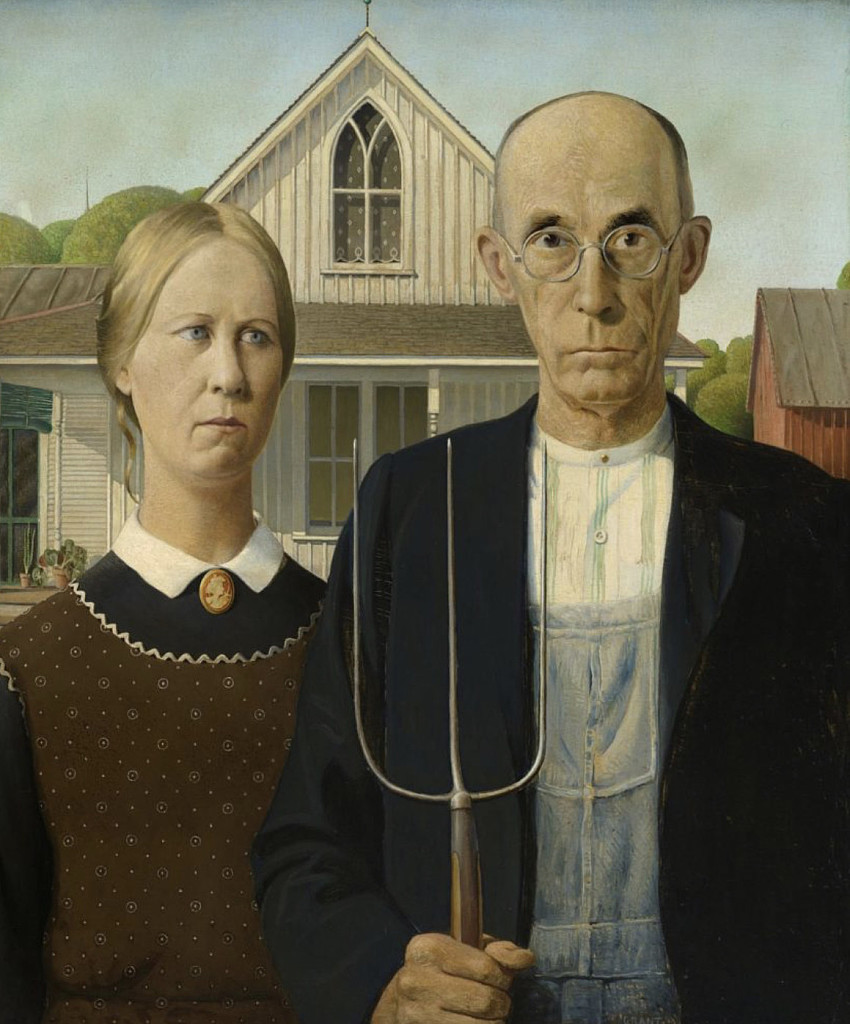
"American Gothic" now hangs at the Art Institute of Chicago. And on the museum's website you'll find a little background information introducing you to the iconic 1930 painting:
The impetus for the painting came while Wood was visiting the small town of Eldon in his native Iowa. There he spotted a little wood farmhouse, with a single oversized window, made in a style called Carpenter Gothic.
"I imagined American Gothic people with their faces stretched out long to go with this American Gothic house,” he said. The highly detailed, polished style and the rigid frontality of the two figures were inspired by Flemish Renaissance art, which Wood studied during his travels to Europe between 1920 and 1926. After returning to settle in Iowa, he became increasingly appreciative of midwestern traditions and culture, which he celebrated in works such as this.
In 1930, Wood entered a competition at The Art Institute of Chicago, submitting American Gothic (a reference to the farmhouse’s architectural style), and won the bronze prize, $300, and, even more essential, widespread accolades, as well as whirlwinds of attention with diverse swirling opinions about the artwork’s meaning.
With the Great Depression roaring across America, this work resonated and gave hope to struggling Americans who sought positive symbols from our hard-working heartland. What emerged, explains curator Haskell, was a profound reverence for values of community and self-reliance — fundamental to our national character, showcased in the USA’s small towns and farms. The painting rocketed Wood’s profile to a nearly mythic level.
Grant Wood died of pancreatic cancer in '42, and his sister eventually moved to Northern California, where she became the caretaker of his legacy. She did, after all, owe him a debt. "Grant made a personality out of me," she said. "I would have had a very drab life without American Gothic."
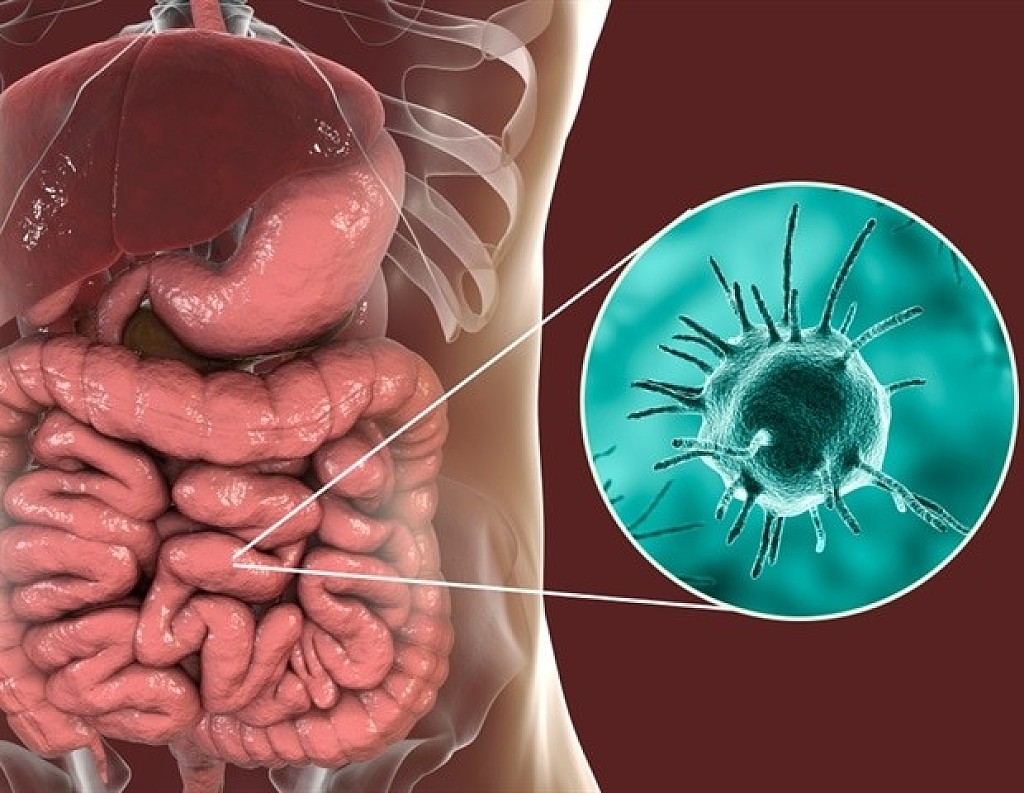
For the first time, researchers from Charité -- Universitätsmedizin Berlin have shown that a unicellular parasite commonly found in the mouth plays a role in both severe tissue inflammation and tissue destruction.
Most patients with severe and recurrent periodontitis (gum disease) showed an increased presence of the amoeba Entamoeba gingivalis inside their oral cavities. The effect of this amoeba is similar to that of Entamoeba histolytica, the parasite responsible for causing amebiasis. Once the parasite has invaded the gingival tissue, it feeds on its cells and causes tissue destruction. According to the researchers' findings, which have been published in the Journal of Dental Research, the two amoebae show similar mechanisms of tissue invasion and elicit a similar immune response in the host.
Periodontitis, or gum disease, is an inflammation of the gums and supporting structures of the teeth. It is one of the most common chronic diseases in the world. In Germany, approximately 15 percent of people are affected by a particularly severe form of this disease. If left untreated, periodontitis will lead to tooth loss.
The disease also increases the risk of arthritis, cardiovascular disease and cancer. In patients with periodontitis, a decrease in the diversity of the oral flora coincides with an increase in the frequency of E. gingivalis. A team of researchers, led by Prof. Dr. Arne Schäfer, Head of the Periodontology Research Unit at Charité's Institute of Dental and Craniofacial Sciences, was able to show that oral inflammation is associated with colonization by the oral parasite E. gingivalis.
Scientists have long been aware of the virulence potential of this genus of amoebae. The gastrointestinal parasite E. histolytica, for instance, causes a disease known as amebiasis, one of the most common causes of death from parasitic diseases worldwide. "We have shown that an amoeba like E. gingivalis, which colonizes the oral cavity, will invade the oral mucosa and destroy gingival tissue. This enables increased numbers of bacteria to invade the host tissue, which further exacerbates inflammation and tissue destruction," says Prof. Schäfer.
The international team of researchers was the first to describe precise roles of E. gingivalis in the pathogenesis of inflammation. During their analysis of inflamed periodontal pockets, the researchers detected evidence of the amoeba in approximately 80 percent of patients with periodontitis, but in only 15 percent of healthy subjects. Their observations revealed that, after invading the gums, the parasites move within the tissue, feeding on and killing host cells. Cell culture experiments showed that infection with E. gingivalis slows the rate at which cells grow, eventually leading to cell death.
The researchers concluded that the amoeba's role in inflammation shows distinct parallels to the pathogenesis of amebiasis. "E. gingivalis actively contributes to cell destruction inside the gingival tissue and stimulates the same host immune response mechanisms as E. histolytica during its invasion of the intestinal mucosa," explains Prof. Schäfer. "This parasite, which is transmitted by simple droplet infection, is one potential cause of severe oral inflammation."
Treatment success is often short-lived in patients with periodontitis. This might be due to the high virulence potential of this previously unnoticed, yet extremely common amoeba. Summing up the results of the research, Prof. Schäfer says: "We identified one infectious parasite whose elimination could improve treatment effectiveness and long-term outcomes in patients with gum disease." He adds: "Current treatment concepts for periodontitis fail to consider the possibility of infection by this parasite or its successful elimination." A clinical trial is underway to determine the extent to which the elimination of this amoeba might improve treatment outcomes in patients with periodontitis.
3D printing is a rapidly growing technology in numerous fields, especially in dental laboratories, all due to the new software, 3D scanners, additive technologies and post-processing methods that increased efficiency and cost savings, to faster production speeds and improved quality to benefit not only doctors but also patients, to make their experience pleasing through the drop of the price, and save time, which is one of the little advantages that this technology brought with it to this industry.
Here are some ways in which 3D printing transformed the dental industry;
Improved Dental Product Quality:
When it comes to manufacturing dentures, 3D printing brings with it a whole host ofpoints of interest. One of the greatest advantages is the improved qualities. Before, With traditional manual workflows, the quality of the finished products is highly dependent on the skills of a given technician. Achieving consistent and high-quality dental products with so many potential sources of error are incredibly difficult and expensive. However, now with 3D printers, even delicate structures can easily be created as the component is built up layer-by-layer and the process is controlled by a software program Compared to a plaster model, a 3D-model is a more stable, durable and precise alternative. The lines and edges on a 3D-model stay sharp without the dental technician having to worry about wearing them down. Compared to a milled model, a 3D-printed model has a more complex structure with a higher level of detail.
Digital technologies simplify workflows, reduce the room for error, and the amount of labor required, resulting in time and cost savings on both the lab’s and practice’s side.
Dental Services are Faster and More Accurate:
With digital dentistry, the room for error is reduced and the automation reduces labor, resulting in time and cost savings for labs and practices all around the world, while Manual model-making is time-consuming while 3D printing allows for multiple appliances to be printed at once since the digital copy is received in minutes because it is sent electronically. The technician can start working as soon as the copy of the scanning arrives. Also, it provides a clean workplace for the technician, without having to deal with plaster or inhale grinding dust.
Accuracy is also improved since 3D printers convert digital images into physical objects by printing 16-micron-thick layers one on top of the other. Increased production capacity and more accurate end results benefit both dentists and patients.
As in all industries, clients always consider the important factor in any business, and the dental industry is no different, especially with the presentation of the new 3D printingtechnology in the industry. As a result, dental 3D printers create models of their patient’s problem areas in preparation for surgery, in order to help prepare themselves for an upcoming surgery reducing anxiety and increasing patient acceptance. In addition, Processes are generally faster as digital elements remove redundant steps, making the patient’s visit quicker and easier, besides that The products themselves can be more aesthetically pleasing and treatments more accurate and less invasive, all of this help to make the client experience way pleasant than it was before, which the patient had to come over a month regularly, and results won’t even be as expected, as a result, the patient end up not happy or satisfied with the outcome.
Saving money is one of the biggest advantages that a 3D printer brought to the dental industry for both patients and doctors, in another word, it’s truly a win-win because the cost of running a dental laboratory can reach $100,000 per year. Compare this to the one-time cost of about $20,000 for a top-model 3D printer, which includes a starting supply of materials. Ongoing materials factor into the lifetime cost, but it’s far lower than running a dental lab. In addition to that, employing skilled staff to produce dental implants presents a considerable ongoing investment. In all, depending on the volume of work. However, Dental professionals aren’t the only ones saving time and money from dental 3D printers. The lower costs of materials and labor mean reduced prices for their patients as well, And with the increased accuracy and speed of dental 3D printers, the amount of return visits needed by patients is significantly reduced.
It is estimated that the overall price of dental care could go down by 80 percent depending on what is needed. In addition, the accuracy level of the work is much higher meaning happier patients.
Exercise has so many documented benefits, including its ability to lower the risk of heart disease, obesity, Type 2 diabetes, and some types of cancer – but research indicates it can also boost oral health. One study published in the Journal of Dentistry showed that regular physical activity can boost periodontal health. To be more precise, people who exercised regularly had a 54% lower likelihood of developing periodontitis compared to those who led sedentary lives. The National Health and Nutrition Examination Survey additionally revealed that people who exercised three times a week or less could also reap benefits, which means they have a 33% lower likelihood of developing periodontitis.
BMI and Oral Health:
There is a vital link between people’s Body Mass Index (BMI) and their dental health. One study published in the Journal of Periodontology found that people who maintain a normal weight and get the recommended amount of exercise had a 40% lower likelihood of having periodontitis. Other health-enhancing behaviors include consuming a healthy, Mediterranean-style diet, which is low in refined sugars and high in fiber, fruits, vegetables, and healthy fats.
Getting Started:
The recommended amount of exercise to boost oral health varies according to age. For most healthy adults, the Department of Health and Human Services recommends around 150 minutes of moderate cardiovascular exercise or 75 minutes of vigorous cardiovascular exercise. Strength training is also key at least twice a week for major muscle groups. People who are starting should do so slowly, increasing workout times and intensities as they progress. Those who lift weights should do so using a trainer-approved workout, using a massaging foam roller to soothe pain. A little pain is to be expected when a person commences weights training in particular, owing to the build-up of lactic acid. Personal pain relief rollers can help, as can stretching and warming up well prior to workouts.
It Works the Other Way Around Too:
We know that exercise can benefit oral health but it works the other way around too. That is, taking care of your teeth can help protect your heart and, therefore, your ability to stay fit and active. A recent study by the European Society of Cardiology found that brushing teeth frequently is linked to a lower risk of atrial fibrillation and heart failure. One possible reason, scientists postulated, is that frequent brushing reduces the amount of bacteria living in the pockets between teeth and gums, thereby keeping the bacteria away from the bloodstream.
Too Much of a Good Thing?
Despite the benefits that exercise can have for oral health, those who train intensively (such as pro or semi-pro athletes) should take note of a Scandinavian study showing that heavy training can contribute to oral health issues, including cavities owing to exercise-induced enamel erosion. Some of the main causes of enamel weakness are drinking acidy sports drinks and breathing with the mouth open during exercise. Athletes can counteract these effects by opting for a water-electrolyte solution, and by aiming to breathe with their mouth closed.
Exercise as a whole is conducive to better oral health – particularly gum health. However, when carried out intensively, it can erode enamel. Rather than give up on exercise, athletes simply need to take care to avoid acidic drinks and to breathe through their nose. Breathing with an open mouth can dry out saliva, thereby leaving the enamel exposed to harmful bacteria.
Oral bacteria are ready to spring into action the moment a dental hygienist finishes scraping plaque off a patient's teeth. Eating sugar or other carbohydrates causes the bacteria to quickly rebuild this tough and sticky biofilm and to produce acids that corrode tooth enamel, leading to cavities. Scientists now report a treatment that could someday stop plaque and cavities from forming in the first place, using a new type of cerium nanoparticle formulation that would be applied to teeth at the dentist's office.
The researchers will present their progress toward this goal today at the American Chemical Society (ACS) Fall 2020 Virtual Meeting & Expo.
The mouth contains more than 700 species of bacteria, says Russell Pesavento, D.D.S., Ph.D., the project's principal investigator. They include beneficial bacteria that help digest food or keep other microbes in check. They also include harmful streptococcal species, including Streptococcus mutans. Soon after a cleaning, these bacteria stick to teeth and begin multiplying. With sugar as an energy source and building block, the microbes gradually form a tough film that can't easily be removed by brushing. As the bacteria continue metabolizing sugar, they make acid byproducts that dissolve tooth enamel, paving the way for cavities.
Dentists and consumers can fight back with products including stannous fluoride to inhibit plaque, and silver nitrate or silver diamine fluoride to stop existing tooth decay. Researchers have also studied nanoparticles made of zinc oxide, copper oxide or silver to treat dental infections. Although bactericidal agents such as these have their place in dentistry, repeated applications could lead to both stained teeth and bacterial resistance, according to Pesavento, who is at the University of Illinois at Chicago. "Also, these agents are not selective, so they kill many types of bacteria in your mouth, even good ones," he explains.
So, Pesavento wanted to find an alternative that wouldn't indiscriminately kill bacteria in the mouth and that would help prevent tooth decay, rather than treat cavities after the fact. He and his research group turned to cerium oxide nanoparticles. Other teams had examined the effects of various types of cerium oxide nanoparticles on microbes, though only a few had looked at their effects on clinically relevant bacteria under initial biofilm formation conditions. Those that did so prepared their nanoparticles via oxidation-reduction reactions or pH-driven precipitation reactions, or bought nanoparticles from commercial sources. Those prior formulations either had no effect or even promoted biofilm growth in lab tests, he says.
But Pesavento persevered because the properties and behavior of nanoparticles depend, at least partially, on how they're prepared. His team produced their nanoparticles by dissolving ceric ammonium nitrate or sulfate salts in water. Other researchers had previously made the particles this way but hadn't tested their effects on biofilms. When the researchers seeded polystyrene plates with S. mutans in growth media and fed the bacteria sugar in the presence of the cerium oxide nanoparticle solution, they found that the formulation reduced biofilm growth by 40% compared to plates without the nanoparticles, though they weren't able to dislodge existing biofilms. Under similar conditions, silver nitrate—a known anti-cavity agent used by dentists—showed no effect on biofilm growth.
"The advantage of our treatment is that it looks to be less harmful to oral bacteria, in many cases not killing them," Pesavento says. Instead, the nanoparticles merely prevented microbes from sticking to polystyrene surfaces and forming adherent biofilms. In addition, the nanoparticles' toxicity and metabolic effects in human oral cells in petri dishes were less than those of silver nitrate.
Pesavento, who was awarded a patent in July, would like to combine the nanoparticles with enamel-strengthening fluoride in a formulation that dentists could paint on a patient's teeth. But, he notes, much work must be done before that concept can be realized. For now, the team is experimenting with coatings to stabilize the nanoparticles at a neutral or slightly basic pH—closer to the pH of saliva and healthier for teeth than the present acidic solution. His team has also begun working with bacteria linked to the development of gingivitis and has found one particular coated nanoparticle that outcompeted stannous fluoride in limiting the formation of adherent biofilms under similar conditions. Pesavento and his team will continue to test the treatment in the presence of other bacterial strains typically present in the mouth, as well as test its effects on human cells of the lower digestive tract to gain a better sense of overall safety for patients.
"Mrs. Klemmedson, Daniel has eight cavities." The pronouncement, made during a boyhood visit to the dentist, remains ingrained in Dr. Daniel Klemmedson's mind.
"I spent way too much time in the dentist's office," said Dr. Klemmedson. In spite of all the time he spent in the dentist’s chair, it was beside the chair where Dr. Klemmedson saw his future. As he remembers it, he was attracted to the convenience.
"I liked the fact that my dentist in Tucson lived in his office," Dr. Klemmedson said. "His office was attached to his house, and I thought that was pretty cool. "What started out as a career of convenience — either be a dentist or marry a dentist — became a passion, layered with greater complexity than what he had imagined as a teenager.
"What other profession allows for full use of intellectual abilities as well as surgical skills?" he asked. "We are the definition of primary care: Diagnosis, education, prevention and clinical care over a lifetime. The autonomy of practice choice, self-regulation and work-life balance cannot be beat."Dr. Klemmedson's career in organized dentistry will culminate Oct. 19 when he is installed as the 157th president of the American Dental Association at the virtual House of Delegates meeting. Because of the COVID-19 pandemic, the ADA Board of Trustees voted to hold the ADA FDC 2020 meeting and subsequently the House of Delegates virtually this year.
'I didn’t know how to stop'Dr. Klemmedson was born in Missoula, Montana, in 1954. His father's job in forestry and watershed management and his doctoral research at the University of California-Berkley forced the family to move around a bit during Dr. Klemmedson's youth: California, Boise, Idaho, and finally, Tucson, Arizona, where Dr. Klemmedson finished junior high, high school and ultimately obtained a bachelor's degree in biology from the University of Arizona.During a college summer, he served as a counselor for Camp Wildcat, a student-run organization at the University of Arizona that provided underprivileged children the opportunity to go camping in the mountains outside Tucson.
It was there he met another counselor: his wife, Adaline. They ultimately married before he started dental school at the University of Southern California in 1976.
Adaline got a job in the fundraising and development division for one of the vice presidents at USC, and benefited from a program to reduce Dr. Klemmedson's dental school tuition by half. A good portion of the remainder of his tuition was paid by the state of Arizona, which had no dental schools at the time so they collaborated with neighboring states to help residents financially.
As a result, Dr. Klemmedson graduated dental school relatively debt free. Without the debt and the stress that typically comes with it, Dr. Klemmedson had a lot more choices when it came to his next steps. His choice? More school."I did not know how to stop," Dr. Klemmedson said.Dr. Klemmedson completed a three-year oral and maxillofacial surgery residency at the Los Angeles County/USC Medical Center in 1983, obtained his medical degree from the University of Southern California School of Medicine in 1985 and completed a transitional internship in the Tucson Hospitals Medical Education Program in 1986.
You read that right: Dr. Klemmedson is a dentist, oral surgeon and M.D.After obtaining all of his degrees, Adaline ultimately put her foot down."Do you like what you do?" she asked. The answer was yes."Then get a job," she responded.
Dr. Klemmedson met his future partners while providing anesthesia for them during a clinical rotation at Tucson Medical Center. Drs. Theodore Kiersch and Edward Schneider were involved in organized oral surgery and invited him to a meeting at the Western Society of Oral and Maxillofacial Surgeons before he joined their practice."One of my partners became a trustee of the American Association of Oral and Maxillofacial Surgeons," said Dr. Klemmedson.
"I was constantly surrounded by organized dentistry and experienced the benefits first-hand."Dr. Klemmedson eventually became president of the Arizona Dental Association, vice chair of the ADA Council on Dental Benefit Programs, a member of the ADA Board of Trustees and now president-elect.He's switched partners a few times and currently has a practice in Tucson and a satellite one in Sierra Vista, Arizona, less than 10 miles from the Mexican border, where many of his patients come from the Fort Huachuca military base or are veterans from the area.For the past 30 years, Dr. Klemmedson has joined primary care and specialty physicians, audiologists, nutrition specialists, sociologists, dentists, orthodontists and oral and maxillofacial surgeons as a member of the Children's Clinics' cleft palate-craniofacial team.
Dr. Klemmedson coordinates surgical care with plastic surgeons and ear, nose and throat surgeons to address the many specific needs his pediatric patients require from birth to adulthood. His primary area of concentration is with the maxillary cleft closure and bone grafting, orthognathic surgery and dentoalveolar surgery.
During the little free time he does have, Dr. Klemmedson "putters around the yard" with his cacti and succulents; exercises every morning at 4:30 a.m.; is an avid cyclist, having ridden across major portions of Australia; and supports his wife's endeavors."My wife, she's kind of the star of the family to be honest," Dr. Klemmedson said. "She leads and I follow."Adaline ultimately became the program director of the Institute for Marine and Coastal Studies at USC.
In Tucson, she also worked in health care, ultimately retiring as a vice president of the teaching hospital associated with the University of Arizona College of Medicine. After retiring, she became a community volunteer and philanthropist "serving as the chair of more local groups in Tucson than I can name," Dr. Klemmedson said.
Dentists will only recommend antibiotics for tooth infections if absolutely necessary.
Dentists will typically only recommend antibiotics in dentistry for tooth infections. However, not all infected teeth require antibiotics.
In some cases, a dentist may simply be able to drain the infected area, remove the infected tooth, or perform a root canal to fix the issue.
They tend to avoid recommending antibiotics unless they are absolutely necessary, such as when the infection is severe or spreading, or if a person has a weakened immune system.
List of types and dosages
Although antibiotics can help clear a tooth infection, it is important to use the appropriate antibiotic in each situation.
The type of antibiotic a dentist recommends will vary depending on the bacteria causing the infection. This is because different antibiotics work in different ways to eliminate different strains of bacteria.
As a study in the Dentistry Journal notes, there are over 150 different strains of bacteria that occur in the mouth. Many of these bacteria have the potential to grow and cause an infection.
Treatment may change depending on the bacteria causing the infection, though much of the time, dentists simply recommend an antibiotic that works against many types.
Penicillin class
Penicillin-type drugs are common forms of antibiotics for tooth infections. This includes penicillin and amoxicillin. Some dentists may also recommend amoxicillin with clavulanic acid, as the combination may help eliminate more stubborn bacteria.
Typical dosages of amoxicillin for a tooth infection are either 500 milligrams (mg) every 8 hours or 1,000 mg every 12 hours.
Typical dosages of amoxicillin with clavulanic acid are around 500–2,000 mg every 8 hours or 2,000 mg every 12 hours, depending on the minimum effective dosage.
However, some bacteria may resist these drugs, making them less effective. In fact, many doctors now choose other antibiotics as their first line of treatment.
Also, some people are allergic to these drugs. Anyone who has had an allergic reaction to similar medications should tell their dentist before receiving their treatment recommendation.
Clindamycin
Clindamycin is effective against a wide range of infectious bacteria. As a study in the International Dental Journal notes, some researchers recommend clindamycin as the drug of choice to treat dental infections, as bacteria may be less likely to resist this drug than penicillin-class drugs.
A typical dosage of clindamycin is either 300 mg or 600 mg every 8 hours, depending on which dosage will be effective.
Azithromycin
Azithromycin works against a wide variety of bacteria, working to halt their growth. It may be effective in treating some tooth infections, though dentists may only recommend it to people who are allergic to penicillin-class drugs or who do not respond to them or other drugs such as clindamycin.
The typical dosage of azithromycin is 500 mg every 24 hours for 3 consecutive days.
Metronidazole
Metronidazole is an antibiotic that doctors and dentists use to treat a number of infections. However, it may not be suitable for everyone and is typically not the first choice of treatment.
The dosage for metronidazole is around 500–750 mg every 8 hours.
Medically reviewed by Dena Westphalen, Pharm.D. — Written by Jon Johnson on June 14, 2019 for Medical News Today
If you want to know how to optimize your oral health during the COVID-19 pandemic, start with your diet.
Loading up on comfort food is, unfortunately, not the best option for your teeth and gums.
To build strong teeth, focus on foods that are low in carbohydrates and sugars, high in fiber, and contain important nutrients your mouth needs, like calcium, phosphorus, and magnesium. Avoid sugary, processed, acidic, and high carbohydrate foods without significant nutritional value.
Let’s take a look at five foods that’ll actively promote oral health:
1. Cacao nibs:
Chocolate is certainly a comfort food, but without added sugar content, it can help prevent cavities by keeping certain oral bacteria in check and stopping plaque from forming on teeth.
A 2009 studyTrusted Source showed that polyphenols in cocoa, as well as certain ones in coffee and tea, successfully kill cavity-causing bacteria and create a barrier between teeth and plaque.
In 2019, researchers found that a cocoa bean mouth rinse destroyed S. mutansTrusted Source bacteria — those most responsible for cavities — equally well to a prescription mouthwash. Even better, there wasn’t evidence that it blasted away other beneficial bacteria in the oral microbiome.
Stick to cacao nibs or dark chocolate with very little to no sugar, as the extra stuff in your average Snickers bar will totally counteract the benefits of the chocolate.
2. Grass-fed dairy:
Grass-fed dairy products, such as cheese and butter, are high in vitamin K2, a nutrient that is vital for healthy teeth. However, a majority of the world’s population is probably vitamin K2 deficientTrusted Source.
While all other mammals can efficiently convert vitamin K1 to K2 in the digestive system, humans don’t have the proper enzyme to make it happen.
And don’t minimize the importance of grass-fed. The enzyme other mammals have is activated by chlorophyll, so animals that live on grain and corn are probably not going to provide a vitamin K2-rich product.
Other high K2 foods that support dental health include natto, beef, goose liver pâté, eggs, and chicken liver. Bonus: Many of these foods are also high in phosphorus, a nutrient that teeth crave.
3. Fatty fish:
Fatty fish is an important component of many healthy diet patterns, as it’s so high in vitamin D. This nutrient is necessary for nearly every system of the body, but one of its lesser-known benefits is its ability to reduce the riskTrusted Source of tooth decay.
Vitamin D works synergistically with vitamins A and K2 to deliver calcium to the teeth, strengthening enamel from the inside out. A deficiency in any of these nutrients can lead to weakened enamel.
Oily fish are also high in omega-3s. Omega-3 fats support gum health and may even help prevent and reduceTrusted Source symptoms of periodontitis (gum disease), which affects nearly half of adults in the United States.
In other words, if your gums regularly bleed when brushing or flossing, consider upping your omega-3 intake to reduce inflammation and bleeding.
Tuna, mackerel, salmon, and trout are some of the fish highest in both vitamin D and omega-3s.
4. Leafy greens:
Greens are beneficial prebiotics within the mouth that healthy oral bacteria feed on. In contrast to high carbohydrate foods, leafy greens help the mouth produce more nitrite-reducing bacteria. In turn, your mouth and cardiovascular system benefit from an increaseTrusted Source in nitric oxide.
Not only will leafy greens leave your teeth feeling cleaner, but they’ll also actively support a healthier oral microbiome.
Darker leafy greens are best for teeth, as they’re also high in minerals your teeth uptake during remineralization to strengthen their structure. Good examples of these include kale, spinach, turnip greens, Swiss chard, and arugula.
5. Grapefruit and oranges:
While acidic foods can have a negative effect on teeth, grapefruit, oranges, and other citrus fruits can actually benefit oral health when eaten in moderation.
Both grapefruit and oranges contain high levels of vitamin C, which strengthens the blood vessels and connective tissues within the mouth. It slows the progression of gum inflammation that could otherwise lead to gum disease.