Although cerebral palsy itself doesn’t cause oral deformities or abnormalities, many of its symptoms lead to oral problems and patients with CP are at a greater risk of dental issues. With diligence and regular dental checkups, however, your child can maintain healthy teeth and gums.
Why Are Children With Cerebral Palsy At Risk for Oral Health Issues?
Some children with cerebral palsy have gastrointestinal reflux and tend to reflux or vomit on a frequent basis. Increased drooling also causes an increased risk of dental caries, as well as some of the medications taken for cerebral palsy may contain high amounts of sugar. All of these factors can lead to a heightened risk of children with cerebral palsy developing tooth decay.
Other issues that heighten the chance of oral problems in children with cerebral palsy include:
Trouble chewing and swallowing, Lack of control when using a toothbrush and floss, Malalignment of the upper and lower teeth, Excessive gagging, Gingivitis due to seizure medications, Having food in the mouth for long periods of time, Lip, tongue, and cheek biting.
Children with cerebral palsy often have problems cleaning their teeth on their own due to jaw muscles that can’t sufficiently relax, mouth and tongue sensitivity, and problems holding a toothbrush and/or floss.
Oral Treatment for Children with Cerebral Palsy
Parents may be hesitant in getting dental care and treatment for a child with cerebral palsy for fear that the visit will be difficult or go poorly. However, there are numerous oral health professionals who specialize in working with children with special needs and make great options for these children.
Safety training is required for all oral health professionals who work with special needs kids, including required training in CPR, training in supporting children with involuntary tremors and bodily movements and training on how to successfully clear breathing passages.
Oral professionals for special needs children are also trained on how to accommodate patients in wheelchairs while providing a calm, child-friendly environment.
Furthermore, oral professionals working with children with cerebral palsy must be trained in how to properly monitor breathing. This is especially important for children who are unable to communicate or have challenges expressing discomfort and pain.
Other qualifications that oral care professionals who work with children with cerebral palsy should have, include:
Ability to establish a trusting relationship with the child, Ability to give commands in a friendly yet understandable manner, Ability to effectively communicate non-verbally (if needed).
The American Dental Association (ADA) suggests that children should start receiving oral health care before they have teeth by wiping their gums down with a warm cloth. This not only cleans their mouth, but it helps them get used to having their mouth cleaned, something that some children with cerebral palsy have difficulties with when they get older.
Once teeth have erupted, regular twice-daily cleaning with a non-fluoridated toothpaste is recommended. Once children are old enough to spit, fluoridated toothpaste is recommended. For children who have difficulty spitting due to cerebral palsy, ask your dentist which type of toothpaste would be best.
Between 18 months to 2 years of age, a child should have his/her first professional dental visit. The dentist will generally check the child’s teeth for any oral issues and teach parents how to help their child care for their teeth at home.
Oral Care at Home
As a parent, guardian, or caregiver, you will be responsible for supervising daily oral hygiene at home. Brushing, flossing, and rinsing should be a daily habit. This includes brushing, flossing, and rinsing after meals and after the medication intake.
“Home dental care and hygiene should be promoted from early on,” the National Institutes of Health reports.
Consider the following to help you become successful with home oral health care for your child:
Purchase toothbrushes and floss that is easier to use, such as an electric toothbrush and toothpick floss sticks, Buy toothpaste made for children with sensitive teeth and gums, Make teeth-cleaning time a fun activity with various child-friendly games and positive reinforcement.
Oral care should be done at a time when the child isn’t tired or angry.
If your child refuses to use a toothbrush, consider using a cotton swab or a warm cloth (consult with your child’s dentist first).
If you need assistance, be certain to speak with your child’s dentist or even a speech therapist who can help you with ensuring your child is swallowing correctly, which makes it easier to keep their mouths clean.
If you find an irritated patch on your tongue, it's tempting to ignore it and hope that it gets better on its own. But if you can't attribute this irritated patch to a specific cause like a burn, abrasion, or trauma, then your condition warrants a trip to the dentist to figure out if it's a sign of something dangerous. Any such oral lesions need to be investigated in case they're a red flag for a precancerous condition. Possible oral lesions include erythroplakia, leukoplakia, or erythroleukoplakia. It's natural to feel overwhelmed, but we're here to guide you through the process. Remember, by not ignoring the red flag, you will help reduce your chances of developing oral cancer.
Definition
According to the American Cancer Society, erythroplakia, leukoplakia, and erythroleukoplakia are terms that describe tissue changes in the mouth.
Erythroplakia. This is a red patch that can be both flat or slightly raised. When scraped, it bleeds easily.
Leukoplakia. This is a white or gray patch.
Erythroleukoplakia. A combination of leukoplakia and erythroplakia, it has both red and white areas.
Causes and Risk Factors
Erythroplakia can be caused by habits like tobacco use or heavy drinking, long-term trauma to oral tissues, or even from aging. While anyone can develop this condition, the risk of cancer increases with age. So, most cases are seen in people over 40 who also exhibit the risk factors discussed above.
Detection
Oral lesions like erythroplakia may initially be painless, but their red appearance warrants further evaluation. So regular examinations of your mouth are critical for early detection.
A dental professional can perform a thorough soft tissue and head and neck exam to detect possible lesions. Research from Jefferson University Hospitals has found that erythroplakia is generally seen on the tongue or the mouth floor. You can also find lesions in the back of the throat and just behind the last molars.
Any areas of suspicion will be examined closely with palpation, gauze, and light and mirrors.
Treatment for Erythroplakia
According to the Oral Cancer Foundation, "verifying the premalignant status of an oral lesion requires a biopsy." Your dental professional or oral surgeon will remove tissue from the area to be sent to a pathology lab for diagnosis. If the results indicate that you have cancer, you will be referred to a specialist for the complete removal of the lesion and the surrounding tissue. If the results suggest that the patch is precancerous, removal or excision may still be recommended.
Taking care of your oral health should include regular dental visits and medical check-ups and practicing good oral hygiene. By paying close attention to your mouth, you can identify possible red flags and reduce oral cancer chances.
Look closely at your front teeth. Between any of them, do you notice gaps that look like tiny black triangles? A dental black triangle occurs when the space between two teeth, also known as an embrasure, is not completely filled by gum tissue. This creates a triangular gap between the teeth and gums.
According to a review in the British Journal of Applied Science & Technology, studies have shown that black triangles can occur in up to 67% of people over the age of 20, making this a rather common condition. However, if not managed properly, these black triangles can lead to more serious oral health issues.
Causes of Black Triangles
Black triangles may result from numerous underlying causes, including a person's dental anatomy and their oral health status. An article in the British Dental Journal (BDJ) notes that some of the most common reasons that embrasures form include:
Older age, Gum disease and recession, Diverging tooth roots following orthodontic treatment, Space between the teeth, Abnormal tooth crown or restoration shape.
Since gum disease can lead to the formation of black triangles, it's equally important to understand the causes of this condition. According to the American Dental Association, there are many contributing factors that may increase one's risk of gum disease, such as:
Not maintaining proper oral hygiene, Genetics, Crooked teeth, which can be hard to keep clean, Using tobacco products, Pregnancy, Diabetes, Certain medications.
Oral Health Risks of Black Triangles
A black triangle is not just an aesthetic problem. As the BDJ article explains, food particles and plaque can accumulate in the gap. The Mayo Clinic notes that plaque accumulation can lead to cavities, as well as more severe oral problems, such as dental abscesses. That's why it's important to get an assessment from a dental professional if you notice these spaces between your teeth.
Treatment Options
Because of the complex nature of the dental black triangle, treatment often requires an interdisciplinary approach. This means that your family dentist may need to coordinate treatment for this condition with various specialists — most likely a periodontist or an orthodontist.
According to the BDJ article, management of black triangles may involve:
Surgical approaches: There are a variety of surgical techniques that can help to preserve the gum tissue between teeth.
Tissue engineering: Tissue engineering involves the injection of regenerative cells to help regrow the missing gum tissue.
Tissue volumizing: Similar to the technique used for facial tissue regeneration, tissue volumizing uses hyaluronic acid to reduce black triangles.
Tooth or restoration reshaping: Altering the shape of the teeth through cosmetic recontouring, bonding or fabricating new crowns or veneers can help to eliminate black triangles.
Pink restorative materials: Pink shades of porcelain and composite materials can sometimes be used to hide or reduce black triangles.
Gingival veneers: A removable gingival veneer or mask is a gum-colored acrylic or silicone device that can be used to cover black triangles. This can be a cost-effective way of temporarily covering the spaces between teeth, but it requires excellent oral hygiene and manual dexterity.
Orthodontic treatment: Although orthodontic treatment can sometimes have the unintended consequence of creating black triangles, it can also help to eliminate the problem in certain cases by repositioning teeth and their roots.
The best way to prevent black triangles from forming between your teeth is to take care of your teeth and gums by brushing twice a day, flossing once daily and visiting your dentist for checkups regularly. While there's no guarantee that you won't see black triangles at some point, you can rest assured knowing that your dental health providers will be able to help you if they appear.
The Mayo Clinic describes epilepsy as a nervous system disorder that causes periods of abnormal activity in the brain. This can affect any process your brain controls, resulting in seizures or changes in behavior or awareness.
Epilepsy can run in families, and other causes include head trauma and brain tumors. In adults over age 35, stroke is a leading cause of epilepsy. In addition, diseases such as meningitis, AIDS and viral encephalitis can also trigger this disorder, as can injuries before birth or other developmental disorders. Despite these known causes, the University of Washington School of Dentistry reports that the exact cause of epilepsy is unknown in 75% of the people diagnosed with this condition.
While it can affect both males and females of all ages and ethnic backgrounds, epilepsy is seen in less than 1% of the population and occurs more often in men.
Common Epilepsy Symptoms
Signs of epilepsy vary, according to the Mayo Clinic; however, a person with epilepsy will most likely have the same type of symptoms with each episode. The following symptoms are usually seen with generalized seizures, which occur when the entire brain is affected:
Temporary confusion, eye blinking or a staring spell, Sudden collapse, Abrupt, uncontrollable jerking or stiffening of the arms and legs, Loss of consciousness.
Oral Health Risks
Generalized seizures create a risk for injuries to your tongue and other areas of the mouth, as the University of Washington School of Dentistry explains. Seizures may also damage the temporomandibular joints or cause an individual to aspirate a tooth into the lungs.
Unfortunately, the drugs used to control this disorder can also produce side effects in the mouth. One side effect often associated with AEDs is gingival hyperplasia, an overgrowth of gum tissue. As an article published in the Journal of Indian Society of Periodontology states, phenytoin is an AED frequently used in children, and it may cause gingival hyperplasia in 50% of the patients who take it.
A study in the Journal of International Oral Health states that AEDs may also cause xerostomia, or dry mouth. Since saliva washes food debris and bacteria from your teeth, dry mouth can make you more susceptible to tooth decay, explains the American Dental Association.
Managing Epilepsy and Oral Health
Since dentures and removable partial prosthetics can break or create a choking hazard during seizures, fixed prosthetics may be a better option for people with epilepsy, according to the University of Washington School of Dentistry. To prevent trauma to the teeth overnight, a dentist may suggest wearing a mouth guard. If a patient develops severe gingival hyperplasia, they may need surgical treatment to remove the excess gum tissue.
A dentist will closely evaluate an epileptic patient for any signs of gingival hyperplasia or dry mouth, and they will share the following oral hygiene steps to help them prevent tooth decay and gum disease:
Floss daily, Brush frequently throughout the day and at bedtime with fluoride toothpaste, Maintain a healthy diet and get adequate nutrition, Use mints or lozenges with xylitol to stimulate saliva production and prevent cavities.
A medical team made up of a doctor and dentist is there to help you or your loved one manage epilepsy. If you're worried about the effects of epilepsy on oral health, know that your dentist is always available to help you keep your smile bright and your teeth and gums healthy.
The U.S. Department of Health and Human Services is amending an emergency declaration under the Public Readiness and Emergency Preparedness Act to authorize additional providers, including dentists and dental students, to vaccinate patients for COVID-19 nationwide, according to a March 11 announcement in the Federal Register.
To date, at least 26 states already enlist dentists to administer the COVID-19 vaccines during the COVID-19 public health emergency. The federal declaration allows licensed dentists throughout the country to vaccinate the public against COVID-19, regardless of state laws that prevent dentists from doing so.
The Association sent a Feb. 11 letter to HHS on this issue and the ADA was also part of a September 2020 coalition letter asking for the same liability protection.“Dentists already have the requisite knowledge and skills to administer vaccines and observe side effects — and many do so on a daily basis,” wrote ADA President Daniel J. Klemmedson, D.D.S., M.D., and ADA Executive Director Kathleen T O’Loughlin, D.M.D., in the February letter. “Dentists are well educated in human anatomy, physiology, and pathophysiology, and are trained to administer intra-oral local anesthesia.
It is arguably more difficult to administer an inferior alveolar nerve block inside the oral cavity than to vaccinate an exposed arm and manage any side effects.”The White House said March 11 the administration will be expanding the pool of qualified professionals able to administer shots to include dentists and other providers. And during his presidential address that night, President Joe Biden announced a goal to make “every adult in the U.S. eligible for vaccination no later than May 1.”
He also vowed to increase the number of places Americans can get vaccinated, including increasing the total number of participating community health centers to 950, and plans to double the number of federally-run mass vaccination centers.The Public Readiness and Emergency Preparedness Act, or PREP Act, allows the Health and Human Services Secretary to issue a declaration in a public health emergency.
This declaration provides temporary immunity from tort liability claims (except willful misconduct) to individuals or organizations involved in the manufacture, distribution or dispensing of medical countermeasures, which may include vaccines. This declaration may be amended as circumstances warrant. During the COVID-19 public health emergency, a declaration was first issued in January 2020 by former HHS Secretary Alex Azar.
On March 11, Acting HHS Secretary Norris Cochran amended the declaration to designate additional health care professionals, including dentists and students, as "qualified persons” whom are authorized to administer COVID-19 vaccines.
Other qualified providers include midwives, paramedics, EMTs, physician assistants, respiratory therapists, podiatrists, optometrists and veterinarians. The amended declaration also includes retired or nonpracticing health care providers who have had active licenses or certifications within the last five years as long as they were in good standing prior to the license becoming inactive, expired or lapsed.
For information about COVID-19 vaccinations, the ADA has created a fact sheet for dentists and dental team members about the status and safety of COVID-19 vaccines. The ADA continues to monitor developments related to COVID-19 vaccine authorization and administration on behalf of the profession and public. Visit ADA.org/virus for the latest information.
If you've been diagnosed with breast cancer and plan to undergo treatment, you probably have many things on your mind. Perhaps the least of which is your oral care. But understanding how chemotherapy and radiation therapy affect your mouth will be pivotal to your oral health during and after treatment. These cancer therapies are incredible, life-saving treatments. But they can come with complications, too, like xerostomia.
Unfortunately, xerostomia is one of the dental problems that can occur with breast cancer treatment. More commonly known as dry mouth, this condition may sound relatively mild, but it can have adverse effects on your oral health. Luckily, there are options for prevention and care! Let's go over the relationship between dry mouth and breast cancer treatment and at-home and professional care you can take to reduce dry mouth. It's important to feel confident about your oral health while you go through cancer treatment!
As you begin to discuss breast cancer treatments with your doctor, you may start to have questions like: Does radiation for breast cancer affect your teeth? What is the relationship between breast cancer radiation and dental treatment? And how can you best protect your smile while going through cancer treatment?
How Likely Is Dry Mouth?
Not everyone develops dry mouth symptoms during breast cancer treatment, but it may occur as a side effect during chemotherapy. Developing dry mouth during chemotherapy may increase your susceptibility to developing oral infections. So it's essential to do your best to maintain oral hygiene during cancer treatment.
Common Complications
Dry mouth can occur during or directly following therapy, and it can usually be reversed. As noted by the American Society of Clinical Oncology (ASCO), a treatment that involves stem cells or a bone marrow transplant can also lead to dry mouth. If your body doesn't respond well to a stem cell or bone marrow transplant, you may develop something called graft-versus-host disease, causing dry mouth.
What Makes Dry Mouth Worse?
While fighting cancer, you may get medications that also have the chance of exacerbating dry mouth. Along with medications that cause dry mouth on their own, chemotherapy and radiation can compound the problem.
Like with other oral health conditions, a poor oral care routine, drinking alcohol, and smoking will make your dry mouth worse. It's also helpful to stop breathing through your mouth to mitigate dry mouth instead of breathing through your nose.
What You Should Do First
At first, it may feel overwhelming to deal with a diagnosis of breast cancer. Dental treatment is probably the last thing on your mind! But it's vital to loop your dental professional into the conversation of care and treatment of your cancer. Be sure to see your dental professional before starting any chemotherapy or radiation. In fact, ASCO recommends you see your dentist at least four weeks before starting treatment for a dental clearance exam. This is so any dental disease can be treated, and your mouth is restored to good oral health, which can prevent oral complications during and after your cancer therapy.
The clearance exam typically includes dental x-rays to diagnose any dental infections. You will also be taught how to care for your mouth during and after your cancer treatment. Your dental professionals will recommend a schedule for future preventive dental care visits, requiring consultation with your oncologist about the appropriate timing during and after your cancer treatment.
How to Combat Dry Mouth at Home
The saliva in our mouths acts as a natural cleanser. It helps wash away food debris and contains properties that neutralize acids, which lead to enamel wear and cavities if left untouched. So when we reduce the amount of saliva in our mouths, this increases the likelihood of developing cavities (dental caries).
You can ultimately help reduce dry mouth complications by staying hydrated and practicing good oral hygiene at home. This includes brushing your teeth twice a day and cleaning between your teeth with floss or a water flosser (also known as interdental cleaning) twice a day. Follow up with mouthwash to wash away any remaining bacteria. Did you know that dry mouth can lead to bad breath later on? That's just one more reason to keep up an excellent oral care routine that makes your breath fresh!
The good news is that there are plenty of ways to reduce dry mouth. They include the following:
Stay hydrated and take sips of water throughout the day, Suck on sugarless candies, Chew sugarless gum, Use a humidifier at night, Avoid smoking, alcohol, caffeine, and other irritants, Drink water along with your meals, Use a lip lubricant, like a lip moisturizer, every few hours, Try over-the-counter saliva substitutes like mouth sprays.
You'll help your body prepare for cancer treatment by maintaining a robust oral health routine and seeing your dental professional for a checkup. By taking these steps, you should feel confident that you're doing everything you can to maintain a clean and strong smile!
If your tongue is larger than what is considered normal, the medical term for your condition is "macroglossia." Here's what you need to know about the causes, symptoms, diagnosis, and treatment of this rare disorder to keep you smiling.
What Are the Causes of Macroglossia?
Macroglossia can be congenital (present from birth) or acquired (developed later in life).
Congenital causes may include various syndromes, like:
Down syndromeA condition in which someone has an extra chromosome.
Beckwith-Wiedemann syndromeA syndrome that causes abnormal growth in different parts of children's bodies and tends to slow at about the age of 8.
MucopolysaccharidosisA condition in which the body cannot break down sugar molecules in the body.
HemangiomaThe abnormal growth of blood vessels usually shows in the form of a birthmark that fades over time. Sometimes it can adversely affect the area of growth, in this case, the tongue.
Congenital hypothyroidismPartial or complete loss of thyroid function. The thyroid gland creates hormones necessary for a variety of things, one of them being growth.
NeurofibromatosisCauses tumors to grow in nerve tissue.
Acquired causes may include conditions or diseases like:
HypothyroidismWith this condition, your thyroid gland doesn't produce enough crucial hormones and can result in a large tongue.
AmyloidosisWhen an abnormal protein called Amyloid builds up and disrupts the function of certain organs in your body, according to Stanford Healthcare, it can also affect the tongue.
AcromegalyYour pituitary gland produces too much growth hormone and typically results in overgrowth of your hands, feet, and face.
Pemphigus VulgarisAn autoimmune disease that can cause swelling and blistering on the tongue.
DiphtheriaA bacterial infection that can be spread through respiratory droplets from coughing or sneezing. It can be prevented with a vaccine.
TuberculosisA bacterial infection that mostly affects the lungs but can also cause lesions and the enlarging of your tongue.
SarcoidosisAn inflammatory disease that usually causes abnormal growths in the lungs, eyes, lymph nodes, and skin but can also affect your tongue.
Symptoms of Macroglossia
If your tongue is proportionally too large for your mouth, you may experience one or more of the following symptoms:
Misaligned teeth
Protruding teeth
Interference with eating
Interference with speaking
Snoring
High-pitched breathing
Diagnosis of Macroglossia
Your medical professional will diagnose macroglossia by performing a physical exam. To determine the underlying cause of the enlarged tongue, appropriate medical testing may be performed. Because there are so many potential causes of this condition, the tests can vary. Your doctor will be able to explain what they recommend for your specific situation and why.
Treatment for Macroglossia
Treatment also varies depending on the cause and severity of your enlarged tongue. If the cause of your macroglossia is both identifiable and treatable, there are medical therapies available. For example, if the cause is determined to be hypothyroidism, treatment for that condition may also help treat your macroglossia. In cases where the cause isn't clear, medical therapies haven't been shown to be useful.
In mild cases of macroglossia, speech therapy may improve issues with speaking. In more severe cases, your healthcare professional may recommend surgery to reduce the size of your tongue. Surgical procedures can help reduce problems with speech, chewing, and feeding.
If you're concerned about an enlarged tongue, see your dental professional or healthcare professional and get their recommendation based on your individual needs. They know your specific circumstances and will be able to advise you on a path of care that will keep you smiling.
The symptoms of an illness may not always be what you expect. A few oral conditions can actually cause what feels like a toothache, when in fact it's something a bit more complicated. If you feel sick, teeth hurt and you want answers, it's worth it to make an appointment with your dentist for deeper insight into the issue. Tooth pain can be connected to a variety of issues, from sinusitis to chest pain.
1. Angina
Angina is a form of chest pain that occurs when not enough blood is able to reach the heart, according to the American Heart Association. It's usually not considered a condition in and of itself, but rather a symptom of coronary artery disease – a much more systemic issue. Interestingly enough, angina doesn't just cause pain in the chest; the Academy of General Dentistry (AGD) suggests it can also cause irritation around the teeth and jaw.
If you have a toothache or jaw pain – or even sharp feelings of stabbing pain, nausea or fatigue, according to Mayo Clinic – it's a good idea to see your doctor. Angina is treatable through lifestyle changes, medications and, in some cases, surgery. Managing it will not only minimize your symptoms, but ultimately help save your life; angina can lead to a heart attack if left untreated.
2. Sinus Infections
If you've been sick, teeth hurt and your nose feels clogged or congested, you might be dealing with a sinus infection. Sinusitis, or inflammation in the sinuses (the hollow cavities in your face), usually occurs after you've been sick with a cold. The buildup of mucus that occurs with a cold creates a great environment for bacteria or viruses to grow.
The sinuses, particularly the maxillary sinus, are located near the upper back teeth. Their proximity to these molars can make it feel as though your teeth hurt when your sinuses are inflamed, according to the Mayo Clinic. Although saline sprays or nasal decongestants can help clear the nose, minimizing any pain, swollen sinuses need to shrink in size for you to feel lasting relief. Use over-the-counter (OTC) anti-inflammatories or similar pain relievers to ease the pain in your teeth and any pressure you might feel in the sinuses.
3. Ear Infections
Just as the location of the sinuses around the tooth can make you feel pain in the teeth when you have a sinus infection, the closeness of the ear to the jaw can cause you to feel pain in your teeth when you have an ear infection. Keep in mind you may develop a toothache on the same side as your ear infection, according to the American Academy of Family Physicians (AAFP). As with sinusitis, however, an ear infection can clear up on its own with time. Feel free to use OTC pain relievers to minimize your discomfort, though.
Whether you have chest pain, ear pain or sinus trouble along with a toothache, it's always a good idea to see a doctor – particularly if the pain persists. Getting an official diagnosis for the illness you have allows your doctor to recommend the best course of treatment for it. He or she can also rule on any actual problems with the tooth itself, such as an abscess or infection, and determine if the pain you feel is connected to your illness.
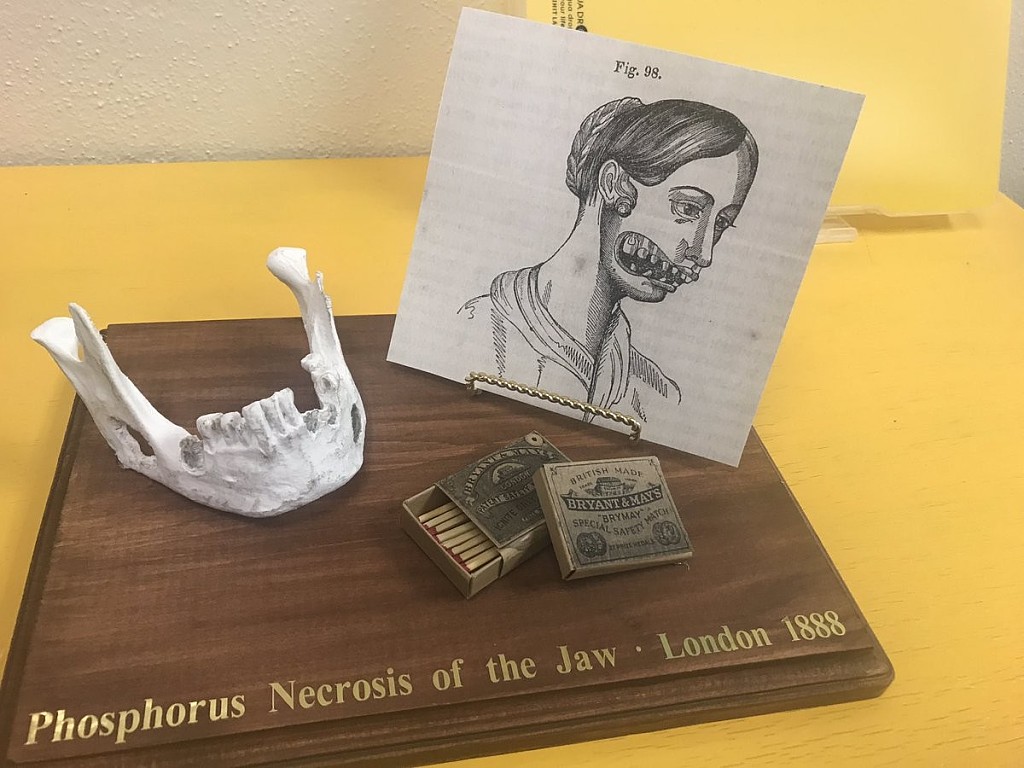
What do household matches have to do with dental health? A look back in time highlights an interesting historical event — which now seems to be repeating itself. In the 19th century, some workers in match factories developed a condition called phossy jaw after being exposed to a chemical used in the match manufacturing process. This condition, clinically known as osteonecrosis of the jaw, vanished until it recently reappeared in the 21st century.
History of Phossy Jaw
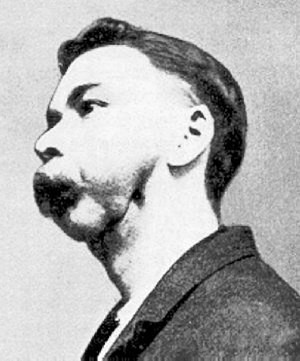
An article in the journal Craniomaxillofacial Trauma & Reconstruction states that this oral disease came about in the 1860s because matchstick factory workers were exposed to dangerous levels of phosphorous — a chemical used for creating matchsticks. Inhaling the phosphorous fumes resulted in a rise in the incidence of gum disease, bone deterioration and bone cell death that was termed phossy jaw.
Beyond the oral effects of this condition, these workers also experienced respiratory symptoms such as coughing, drainage and bloody discharge from the lungs that was termed phossy lung. They also experienced seizure conditions called phossy brain and blood conditions known as phossy marrow. These toxic responses were all eventually traced back to the matchstick factories, and the condition soon disappeared among the population after alternative factory materials were introduced in 1906.
Modern-Day Phossy Jaw
To understand why cases similar to phossy jaw have returned, you'll first need to understand how bisphosphonates work. As Johns Hopkins Medicine explains, doctors often prescribe bisphosphonate medications to patients with systemic diseases such as osteoporosis, which is a condition that weakens the bones. These medications prevent and treat bone thinning in individuals who are diagnosed with osteoporosis, lupus or other bone-weakening conditions. Bisphosphonates work by slowing the process by which the body dissolves certain bone-building minerals.
Despite this medication's positive effects, one possible side effect of using bisphosphonate drugs is bisphosphonate-induced osteonecrosis of the jaw (ONJ), which is very similar to phossy jaw. The American College of Rheumatology (ACR) describes ONJ as a condition where the jawbone becomes exposed and doesn't get enough blood, so it begins to weaken and die, often causing pain. An individual who is taking or has previously taken bisphosphonate medication is at a greater risk for ONJ, and it most commonly occurs following dental extractions.
It's common for dental professionals to advise patients who need extractions to discontinue the use of bisphosphonate drugs and take an antibiotic prior to the procedure, explains Johns Hopkins Medicine. This is because, while bisphosphonates are used to prevent bone thinning, they can interfere with jawbone healing, especially after dental work.
Bisphosphonate-induced ONJ is rare, as the National Osteoporosis Foundation notes. But ONJ can also occur in individuals who have not taken bisphosphonate drugs. Other risk factors for ONJ include radiation treatment, infection and steroid use.
Treating and Preventing Osteonecrosis of the Jaw
The ACR says that patients who have taken bisphosphonates or are currently taking them should inform their dental provider of their medication history prior to any dental care. This allows the dental provider to take precautions should a surgical procedure be necessary — especially in cases of tooth removal. If an individual does develop ONJ, their dental professional will likely recommend antibiotics, oral analgesics and mouthrinses, which are often effective.
Both dentists and oral and maxillofacial surgeons know how to identify the risk factors associated with using bisphosphonate medications, thanks to their dental school education and extensive training. When you keep your dental professionals informed about your medication use, they can plan their approach accordingly to help prevent ONJ and other healing complexities following dental treatment.
A coronectomy is a dental procedure that’s done in certain situations as an alternative to having a wisdom tooth extraction.
A coronectomy can be done when a dentist feels there’s an increased risk of injury to the inferior dental nerve. It may also be considered safer than an extraction in people over 40, according to some researchers.
Coronectomy vs. extraction
A standard wisdom tooth extraction will remove the entire tooth, and sometimes all four are removed at once. A coronectomy will remove the crown of the tooth and leave the tooth’s roots in your jaw, intact.
A coronectomy isn’t recommended if the wisdom tooth or root is infected.
Both procedures may be done by a dentist or oral surgeon. Your dentist will likely decide on one procedure over the other depending on factors such as your age and likelihood of nerve damage.
Why have a coronectomy?
Sometimes the wisdom teeth roots are close to, press on, or even wrap around your lingual nerve (LN) or inferior alveolar nerve (IAN), the nerves that supply feeling to your tongue, lips, and chin.
In situations like this, your dentist or oral surgeon might recommend a coronectomy as an option that could lower risk for potential nerve damage as compared to an extraction.
Damage to your LN and IAN might result in:
pain or odd sensations in your lower lip, lower teeth, lower jaw, or chin
difficulties speaking
difficulties chewing
loss of taste
According to a 2015 reviewTrusted Source, extracting a wisdom tooth with roots near the IAN can cause direct or indirect damage to the nerve. Coronectomy in that situation can be a safe procedure that’s associated with a low incidence of injury to the lingual or inferior alveolar nerves.
According to other research from 2015Trusted Source, a coronectomy is preferable to extraction for preventing neurological damage when roots are near the IAN.
What to expect following a coronectomy
Following your coronectomy, you’ll probably have some swelling and discomfort, although usually less than you would after a full extraction.
Your dentist will provide aftercare instructions and might prescribe antibiotics, although the risks of postoperative infection and dry socket is reduced as compared to extraction.
As with any dental procedure, if you notice any signs of infection, excessive bleeding, or other unusual symptoms, you should call your dentist or oral surgeon.
When a coronectomy isn’t recommended
Typically a coronectomy is used when the tooth that needs to be removed has roots that are near important nerves. There are specific situations when a coronectomy is usually not recommended, such as: