Can a probiotic derived from Chinese pickles prevent cavities? That seems to be the case, according to a study by researchers at Ben-Gurion University of the Negev and Chengdu University in China.
Pickles are an integral part of the diet in the southwest of China. When fruits and vegetables are fermented, healthy bacteria break down the natural sugars. These bacteria, also known as probiotics, not only preserve foods but offer numerous benefits, including immune system regulation, stabilization of the intestinal microbiota, reducing cholesterol levels, and now inhibiting tooth decay.
According to the study published in Frontiers in Microbiology, a strain of Lactobacilli (L. plantarum K41) found in Sichuan pickles reduced S. mutans by 98.4%. Dental caries (cavities) are caused by Streptococcus mutans, (S. mutans) commonly found in the human oral cavity as plaque and is a significant contributor to tooth decay.
Prof. Ariel Kushmaro of the BGU Avram and Stella Goldstein-Goren Department of Biotechnology Engineering and the Chinese research team evaluated 14 different types of Sichuan pickles from southwest China. They extracted 54 different strains of Lactobacilli and found that one, L. plantarum K41, significantly reduced the incidence and severity of cavities. K41 was also highly tolerant of acids and salts, an additional benefit as a probiotic for harsh oral conditions. It also could have potential commercial value when added to dairy products.
According to Doug Seserman, chief executive officer of American Associates, Ben-Gurion University of the Negev based in New York City, "the researchers currently have no plans to evaluate Jewish deli pickles."
Have you ever given thought to how what you eat and drink can affect your oral health? Two of the most prevalent diseases, tooth decay, and periodontal or gum disease, may be preventable by changing your diet. Decay is a result of acids produced by oral bacteria destroying your teeth and other hard tissues of the mouth.
What Food and Drinks Should I Avoid?
Certain foods and drinks will leave you at a higher risk for dental problems. Although acidic foods, such as lemons and limes, may be delicious, frequent exposure can erode your enamel. The erosion will lead to tooth decay and potentially periodontal disease.
When you are snacking, try to avoid soft, sweet, and sticky foods that will cling to your teeth and promote tooth decay. You may end up at a higher risk of dental problems, such as tooth decay in comparison to other snacks.
Avoid drinks that contain sugar, as they allow the sugar molecules to coat your teeth and hide in hard to reach areas. Limit your alcohol consumption as it causes a reduction in the flow of saliva, leading to tooth decay and other oral infections.
Did you know that heavy alcohol use increases your risk for mouth cancer?
Preventative Care:
To give your body the nutrients it needs to keep your teeth strong, consume a well-balanced diet that is characterized by moderation and variety. Keeping your mouth moist by drinking water throughout the day will allow a greater production of saliva, protecting both hard and soft oral tissues.
The plaque, a mass of bacteria, that grows on your teeth thrives on sugar so do your best to avoid sugary foods and drinks. The times that you cannot avoid sugar, simply brush your teeth after your snack or meal. Try to limit the amount of time sugary treats remain in your mouth!
Remember to brush your teeth at least twice a day and floss regularly to prevent dental problems! Don’t forget to get your teeth cleaned professionally to leave your mouth, clean, fresh, and less prone to disease.
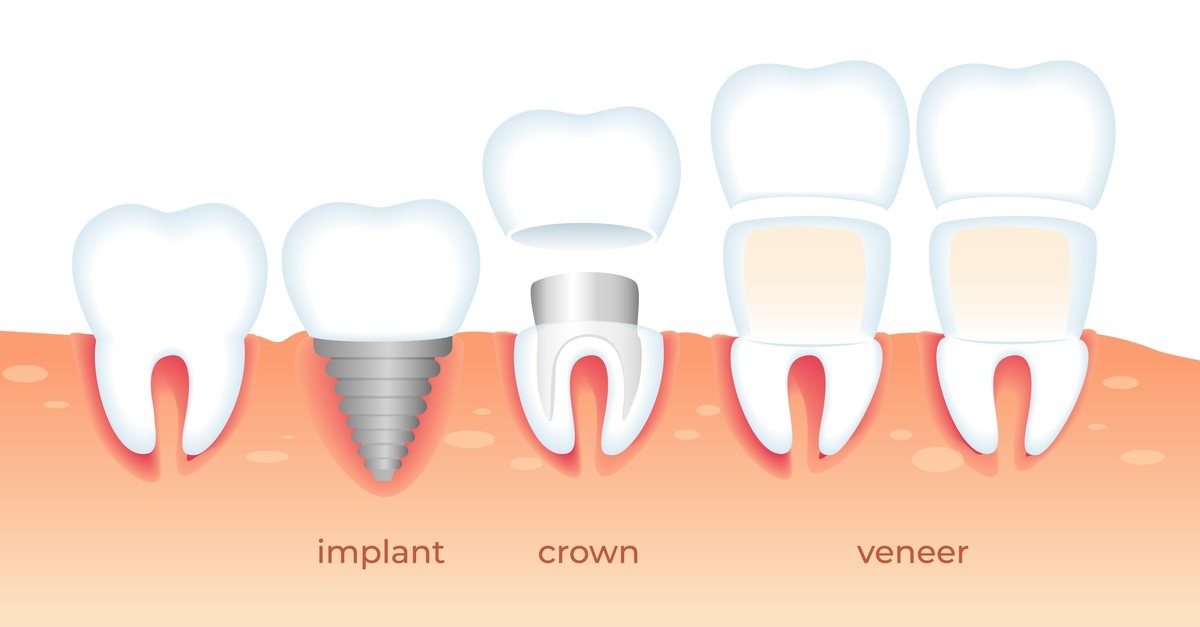
Dental veneers, crowns, and implants can all improve the cosmetic appearance of the teeth. However, there are differences between them.
One difference between veneers, crowns, and implants is the area of the tooth that each option covers.
Dental veneers mainly cover the front of a tooth. By contrast, crowns cover the entire tooth, including the front, back, and all the sides. As a result, dentists use crowns to repair broken teeth, including teeth that have little structure left. Crowns can also help strengthen the teeth they cover.
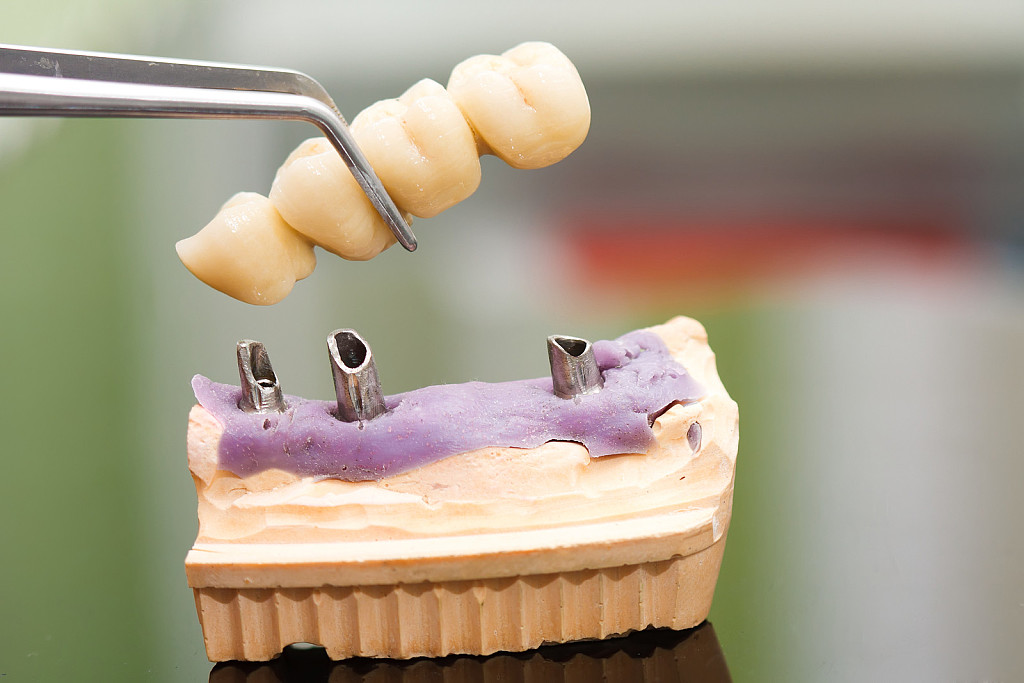
Implants, meanwhile, are bolt-like structures that attach to the jawbone to replace missing teeth.
When necessary, a dentist may use an implant to secure a crown in the mouth. This may be the case if a person is missing a tooth or a tooth is irreparable because it is too badly broken down and requires removal.
Essentially, dentists use crowns to build up teeth that are badly damaged, whereas implants replace missing teeth. Veneers improve the appearance of teeth that are mostly still intact.
What happens during the dental veneer procedure?
According to the ADA, how the dental veneer procedure goes depends on the type of veneer a person chooses.
The following sections will outline the process for each type below.
Porcelain veneers:
To fit porcelain veneers, a dentist will first remove some enamel and take an impression of the teeth to create a mold.
After this initial visit, they will send the mold to a laboratory that fabricates the custom-fit porcelain veneers. The dentist may place temporary veneers on the teeth while a person waits for the laboratory to make the permanent ones.
At the next appointment, the dentist will test whether or not the veneers fit and are a good color, and they will make any adjustments as needed. Then, the dentist will bond the veneers to the teeth.
Resin-based composite veneers:
To fit resin-based composite veneers, the dentist will start by cleaning, reshaping, and preparing the teeth. After they prepare the teeth, they will bond and sculpt the composite material, adjusting the color so that the veneers look natural in the person’s mouth.
Then, the dentist will use a light to dry and harden the composite material. Once the veneers have hardened, the dentist will smooth and polish them so that they look and feel like real teeth.
Aftercare:
After the placement of veneers, the dentist may want to check them in a follow-up appointment. During this, they will look to make sure that the veneers have stayed in place and are comfortable for the wearer.
This is a good opportunity for a person to mention if any of the veneers do not feel right, as a dentist can help fix them.
A person with new dental veneers does not need to avoid any particular foods or beverages following their appointment.
That said, because veneers may stain over time, a person may want to avoid coffee, tea, and red wine, as well as other things that can cause stained teeth, to make them last longer.
The dentist may also advise against:
1. biting hard objects.
2. biting the nails.
3. using a mouthguard.
4. grinding the teeth.
5. chewing very hard foods.
6. opening items with the teeth.
Also, a person can still develop cavities even though they have veneers, so it is important to practice good oral hygiene, including brushing the teeth twice per day and flossing daily.
With the right care, a person can expect their veneers to last around 10 years. After this time, a person may need to replace them.
Here is an overview of the differences between each dental solution:
Dental Crowns:
Restore a damaged tooth by covering it with a porcelain cap.
For cosmetic and restorative purposes.
Dental Bridge:
Used to replace one or more missing teeth.
Can be fitted with dental crowns or implants.
For cosmetic and restorative purposes.
Dental Implant:
A fully functional tooth replacement that is embedded into the jaw.
Can be installed with a bridge to replace multiple missing teeth.
For cosmetic and restorative purposes.
Dental Veneer:
A coating used to reshape or brighten teeth that are misshapen or discolored.
Primarily used for cosmetic purposes, but can be restorative.
Dr. Marine Martirosyan is a recognized Cosmetic Dentist in Glendale, CA. She received her degree from the prestigious University of Southern California in 1996. A powerful education and doctoral training provide her with the foundation of knowledge and experience necessary to bring the latest breakthroughs in the field of Cosmetic Dentistry to her dental practice located in Glendale.
In addition to caring for patients and providing the best dental experience, Dr. Marine’s hobbies include painting. Here is some of her art work. She is showing 67 more of her pieces on her website.
She is passionate about her profession and this is reflected through the beautiful smiles she creates. She strives to give her patients the smile of their dreams, and makes them look and feel great! She blends professionalism and a care to give you the smile you deserve.
Dr. Martirosyan has high standards of care and attention to every detail in her work at her dental office in Glendale, giving you a smile like no one else.
Dr. Martirosyan serves a broad area of dentistry, specializing in all cosmetic dentistry procedures. She is considered to be one of the most talented cosmetic dentists in Los Angeles, let alone the best cosmetic dentist in Glendale 91202 and a unique cosmetic dentist in Burbank. Compared to most cosmetic dentists in Glendale, she offers more than your average dentist’s office.
Her dental office in Glendale uses the latest technology and techniques for cosmetic dentistry. We offer an excellent track record in the following cosmetic dentistry techniques and more.
She posted this on her website, "In order to protect the health of our patients and staff, we have implemented heightened safety protocols, including increased infection control and sanitation measures."
She purchased Universal Gowns from PPE by UjENA for her practice.
Michael Adler’s headgear provokes all kinds of comments. You’ve seen heath care workers wearing face shields during the coronavirus pandemic. Adler, a dentist who co-owns Adler Family Dental in Aberdeen New Jersey with his brother Eric, wears a face shield surrounded by black casing.
It's a full helmet.
“People call me Darth Vader,” he said. “Or they say, ‘Where’s your Harley?’ But this is how I feel safe.”
The Adlers said they spent $30,000 on safety upgrades since March.
Michael’s helmet is the most obvious example, but there’s more. They installed a UV light air sanitizer into their office’s HVAC duct system, placed air purifiers in each treatment room and brought in Pax2000 Extraoral Dental Suction units, which are designed to remove droplets and aerosol particles created during dental procedures.
(First photo) Eric Adler and Michael Adler don their PPE at Adler Family Dental in Aberdeen NJ.
“In each treatment room we’re managing the air around the patients,” said Eric Adler, who is also a dentist. “The name of the game is managing the air quality.”
So the Adlers, like many in their profession, were taken aback last week when the World Health Organization advised people to delay routine dental appointments in areas with COVID-19 community spread.
“The WHO is out of line,” Michael Adler said. “We’re safer in our office than they are in their own offices.”
On Tuesday the WHO clarified its guidance, saying routine appointments should be delayed only in areas with “intense, uncontrolled community transmission.”
To date, according to the Centers for Disease Control and Prevention, there have been no reported cases of COVID-19 clusters traced to dental offices in the United States.
“To me, that even suggests that protective equipment used prior to COVID-19 was perfectly suitable,” said Art Meisel, executive director of the New Jersey Dental Association. “Now, extreme precautions are being taken.”
At the direction of Gov. Phil Murphy, the Adlers closed their practice to all but emergency appointments from March 17 to May 26, during which time it underwent a complete makeover.
“We had 628 patients that had scheduled cleanings that did not get seen,” Michael Adler said. “When we reopened, the phones were ringing of the hook. We had to work six days a week at expanded hours just to accommodate the demand.”
Because some other dentist’s offices in the area have not yet reopened for various reasons, Michael Adler estimated “we are probably at 110% of our previous work level.”
Speaking broadly, Meisel estimated “the numbers are back to about 80% in most offices.”
Between the additional safety costs, the appointments lost to closure and the need for a wholesale reimagining of patient interaction, “these have been tough times” for the dental profession, Meisel said.
Not to mention an entire society living on edge.
“It’s a pandemic; everyone has some level of anxiety,” said Michael Adler, a father of three who lives in Marlboro. “I have two 12-year-olds and an 8-year-old I come home to every day.”
That’s why he puts on the helmet. It works for him and for his patients.
“It’s been challenging,” he said, “but also very rewarding to know we’re absolutely needed to help promote oral health.”
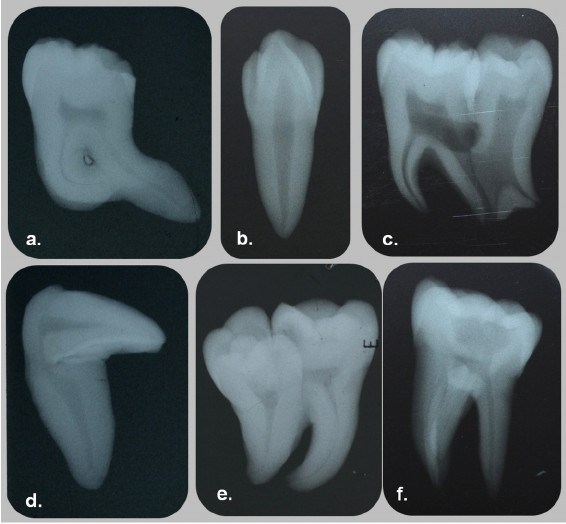
Some form of dental anomalies, or at least dental irregularity is found in nearly every individual, including men, women and children. Some of these are relatively mild and simple, as in rotations of teeth, small interdental spacing and unusually shaped teeth. Others are more complex and cause more functional and esthetic concerns. Among the latter, one should include congenitally missing, impacted and severely crowded teeth and also craniofacial anomalies, such as various forms of clefts. An orthodontist, who is primarily concerned with the function and esthetic of the human dentition, sees these dental anomalies as a challenge in his efforts to change a malocclusion to a more normal and cosmetic occlusion.
Traits of Malocclusion
It is well accepted that among all the traits of malocclusions of the modern man, dental crowding is the most preva- lent, possibly second only to the rotation of an individual tooth. For that reason, it is not surprising that dental crowding occupies a central place in this specialty’s discussions about etiology and pathogenesis of malocclusions. It could be well speculated that if practitioners understood the mechanisms of crowding, they could be able, at some point, to intercept or even prevent it and thus substantially reduce the incidence of malocclusion in the modern population. However, the way things stand right now it is not very likely that this important public health issue will be affected any time soon.
Second to dental crowding, anomalies in the number of teeth represent a large group of primary factors causing malocclusions. This is closely followed by an anomalous position of teeth, chiefly represented by impactions and ectopic eruption, but also including transpositions and transmigrations. Therefore, these etiologic factors should also be looked at in an effort to understand and reduce or even eliminate them in the future. Consequently, it is necessary to revisit some of the salient features of these anomalies. Particularly challenging will be to summarize the recent investigative reports in this area, as well as to speculate where future research should be directed. Once we are able to substantially reduce these underlying dental anomalies, we will be well equipped and ready to tackle even more complex cranio-facial problems.
Etiology and pathogenesis of dental crowding
There are two basic mechanisms in creating the condition that we refer to as dental crowding. By definition, crowding is a discrepancy between the cumulative widths of the dental units or teeth, and the available space to accommodate these teeth within the alveolar bone. Thus, one can represent a ratio between the tooth size and the supporting bone size. When this ratio exceeds unity, we define such a condition as dental crowding. If the ratio is one or less than unity, we don’t speak about dental crowding, but may, in fact, identify the condition as dental spacing. Arguably, crowding exceeds spacing by a large margin, perhaps as large as 100 or more to one. The ratio of exact unity or one is so rare in real life that it can, for all practical purposes, be ignored.
It is generally recognized that the most common positional anomaly of a tooth is rotation. Rotations are so prevalent that it is difficult to find a modern man or woman with an occlusion that does not exhibit some degree of this common anomaly. Because this anomaly is so ubiquitous, many clinicians do not even list them as a trait of malocclusion, except when rotations are severe, e.g. a Orthodontics tooth rotated more than 45 degrees.
From the clinical aspect, rotations are not overly difficult to correct, particular- ly with the use of fixed orthodontic appliances. It is important to keep in mind, however, that corrected rotations also represent the condition most likely to relapse. Various strategies have been developed to guard against, or to minimize, rotational relapse. One of the most effective ones is the procedure known as supra-crestal fiberotomy [SCF], a minor surgical procedure in which the supra-crestal gingival fibers are sev- ered.4
Ectopic position constitutes the second most common positional anomaly of the dentition. Within this category, the one that concerns clinicians the most is impaction. Even though any one tooth from either dental arch can be impacted, impaction of the maxillary permanent canine receives most attention. This is the case for numerous reasons, including the central role that the canine plays in the function of articulation and occlusion. A second, nearly equally important reason, is its role in facial esthetics.
A brief mention will be made of yet another positional anomaly of the canines: transmigration. Transmigration is exclusive of the mandibular perma- nent canine. In this anomaly, the canine from one side of the arch migrates through the bone and erupts on the opposite side of the arch. For instance, the right mandibular canine migrates through the sympheseal area and erupts into the arch in the place where the left canine usually erupts. This anomaly could present a complex clinical problem, because the clinician will be facing a situation where the canine from one side appears to be missing, while the opposite side may appear to have a supernumerary canine.15 Like so many dental problems, this last anomaly is best detected by radiographic examination. If detected early enough, its treatment may not be too difficult. This will reinforce the urging of a mature teacher to obtain and examine our patients’ records with care and attention to detail.
A clinician faces a large variety of dental anomalies in his or her everyday work. This review dealt with only the most common ones that particularly affect an orthodontist. A better understanding of these will make the work of a clinician more efficient and perhaps a bit more enjoyable.
A study conducted at a hospital in Tokyo has found that poor oral hygiene could lead to prolonged viral shedding in patients with COVID-19. In the study, it was observed that patients with inadequate oral health regimes returned positive results in polymerase chain reaction (PCR) tests for the virus long after their clinical recovery, leading the researchers to believe that oral hygiene could affect the accuracy of testing for the virus.
The researchers evaluated the course of treatment of eight COVID-19 patients who were admitted to the Department of Neurology at Tokyo Metropolitan Neurological Hospital between 30 April and 14 May. The patients had passed the acute phase of the disease, but were admitted to the dedicated medical facility for infectious diseases owing to persistent positive PCR test results for SARS-CoV-2.
The study found that, among the patients, the viral shedding period—the period during which the virus was still detectable after clinical recovery—ranged from one to 40 days. The average viral shedding period was found to be 15.1 days, but for two patients, Patient 1 and Patient 2, it continued for 53.0 days and 44.0 days, respectively. For Patients 3–8, two consecutive negative PCR test results were confirmed within 18 days of clinical recovery.
The researchers sought to establish why Patients 1 and 2 continued to test positive for the extended period. They noted that Patients 3–8 had kept up their personal hygiene routines, which included regular toothbrushing, while hospitalised in isolation in private rooms in the hospital. Patients 1 and 2, however, who had mental and/or psychiatric disorders, had not voluntarily brushed their teeth while hospitalised. After being instructed by the researchers to practise regular toothbrushing and gargling, the PCR tests of Patients 1 and 2 returned a negative result within four to nine days.
“Patient 1 had schizophrenia and was unable to voluntarily keep herself clean during isolated hospitalised life,” the study reads. “She brushed her teeth for the first time on the 18th day of hospitalisation, but after that, she did not brush her teeth at all. Her virus shedding period reached 46 days, with consistently positive PCR test results. We speculated that her inappropriate oral care might have caused the persistence of PCR test positivity. In collaboration with the nurse, we repeatedly encouraged Patient 1 to brush her teeth and gargle. Two days after the start of this instruction, on the 49th day after the patient’s onset of symptoms, the patient’s PCR test result was negative for the first time.”
Patient 2, who had the underlying diseases of dissociative disorder and mild mental retardation, returned a negative PCR test result 26 days after being admitted to the medical facility; however, the viral shedding period reached 43 days before two consecutive negative PCR test results could be obtained. “At that time, we found that Patient 2 rarely brushed her teeth. Since then, we repeatedly instructed her to brush her teeth. With four days of intensive toothbrushing with only water, Patient 2 had two consecutive negative PCR test results on Days 44 and 47, so she was discharged,” the researchers wrote.
They acknowledged that the low number of patients who were followed in the study made it difficult to draw statistical conclusions from the research, but noted that it was significant that the two patients with poor oral health regimes had displayed significantly longer than average viral shedding periods. “In such prolonged viral shedding cases, non-infectious viral nucleic acid may accumulate in an uncleaned oral cavity and may continue to be detected by PCR. We propose toothbrushing and gargling to remove accumulated non-infectious viral nucleic acid, leading to consistently negative PCR test results and thus avoiding unnecessarily long hospital stays,” the researchers concluded.
The study, titled “Effects of oral care on prolonged viral shedding in coronavirus disease 2019 (COVID-19)”, was published online on 24 July 2020 in Special Care in Dentistry, ahead of inclusion in an issue.
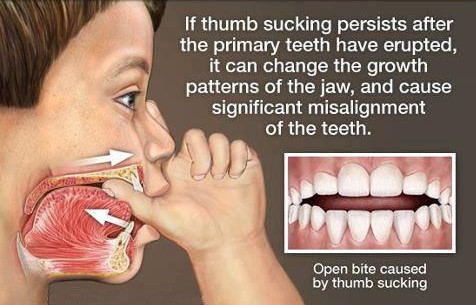
During infancy it is common for babies to explore the world using their mouths, this is a natural instinct that babies are born with, and all parents know how stressful this can be! Sucking on a pacifier, thumb or fingers is perfectly normal for the first few years of life, as children use this to help themselves feel calm and reassured.
However, if this continues beyond 5 years of age, it could be a sign of a problem with a child’s emotional or social development. Helping your child break the habit at the right time is important, otherwise this could have some unwanted side effects.
Possible side effects:
One of the main benefits to both child and parents of this habit is that it helps them both fall and stay asleep much more easily. However, starting to break the habit before your child’s teeth begin to develop is really important, as if they are allowed to continue, this could cause problems with their teeth alignment which could give rise to the need for dental work in the future.
If a child is still sucking on their thumb or pacifier after they have developed all their milk teeth, then this has the potential to lead to middle ear infections which could in some cases end up in needing surgery.
Other long-term effects of excessive thumb sucking include:
1. The development of an underbite or overbite
2. Malformation or sensitivity of the roof of the mouth
3. An adverse effect on jaw positioning which could lead to a speech impediment
4. An increased chance of picking up harmful bacteria or pathogens
5. Skin problems such as a thumb callous or warped thumb nail
6. Social issues such as being bullied by their peers.
How to break the habit:
About 30% of children in pre-school still suck their thumbs, however the following advice could help you ensure that your child breaks the habit at a healthy time. The most important thing is to show support and positive encouragement to your child while they are in the process of stopping, this will help build their self-esteem which will in turn reduce the need or desire to suck their thumbs for comfort.
Educate them on the reasons to stop:
Taking the punishment route or continually nagging them could cause them stress which will in turn make them want to suck their thumbs more. Eliminating any stressors in their environment will also help encourage them to stop. Educating your child on the risks and potential long-term effects of continuing the habit will make clear to them the reasons why they should stop and hopefully help put them off.
If the situation still isn’t improving there are other less pleasant routes that you can go down such as putting socks on your child’s hands while they sleep and using tape to keep them in place, or asking your dentist to prescribe a bitter-tasting medication to put on the end of their pacifier or thumb which will make it very unpleasant for them.
How to wean your child off their pacifier:
If your child is still sucking a pacifier at 5 years of age then another method is to cut the pacifier shorter or pierce a whole through it, this will make the pacifier much less satisfying to suck which will reduce their desire for it. For some parents, simply just going cold turkey or leaving the pacifier at home when going on a trip is enough.
In summary, there are a range of interventions that you can try, and the idea is to start with the softer less invasive methods first. But be reassured that you will be able to find at least one solution that will work, and even though it may be unpleasant in the process, it will be worth it in the long run.
Obesity and gum (periodontal) disease are among the most common non-communicable diseases in the United States -- and studies show these chronic conditions may be related. This new study explores the effect of obesity on non-surgical periodontal care and evaluates potential pathways that may illustrate the connection between the two conditions.
The connection between obesity and gum disease isn't as simple as cause-and-effect, said Andres Pinto, professor of oral and maxillofacial medicine and diagnostic sciences at the Case Western Reserve University School of Dental Medicine and co-author of the study published in the British Dental Journal.
Instead, the relationship centers on what both diseases have in common: inflammation.
Examining a plethora of existing studies, researchers found that data showing increased body mass index, waist circumference and percentage of body fat to be associated with an increased risk to develop gum disease, also known as periodontitis. Most studies analyzed data from population subsets at one point in time, as opposed to studying the same population over a longer period.
They concluded that changes in body chemistry affect metabolism, which, in turn causes inflammation -- something present in both maladies.
"Periodontal disease occurs in patients more susceptible to inflammation -- who are also more susceptible to obesity," Pinto said.
This information can inform how health-care professionals plan treatments for patients suffering from obesity and/or gum disease, Pinto said.
"Oral health-care professionals need to be aware of the complexity of obesity to counsel their patients about the importance of an appropriate body weight and maintaining good oral hygiene," he said.
Pinto said further research on the relationship between gum disease and obesity is needed, noting there is, at this point, limited evidence to recommend changes in treatment planning.
"There is a thought, from the clinical perspective, that if you treat one of the issues, it may impact the other," he said. "This is the big question. For example, if we treat obesity successfully, will this impact periodontal disease to the point of being of clinical relevance compared to control population. The jury is still out given the paucity of controlled, well designed, clinical trials on this issue."
Dental diode lasers have already proved their worth in many dental treatments, compared to conventional treatment methods. With the development of blue laser light with a wavelength of 445 nm, lasers now cover an even greater range of treatments than ever before.
The French dental practitioner Dr. Carlos Sfeir reports on his experience with the blue wavelength.
Lasers have been used in dentistry since the 1990s. It has now become an established treatment method, which is certainly due in part to its large range of indications. Whether for surgery, treatment of the peri-implantis or even for medical bleaching – exciting progress in treatment and diagnostics has been achieved due to the ongoing development of dental lasers.
With their diverse spectrum of applications, diode lasers in particular have been widely adopted over the years.
At my practice in Sillé le Guillaume in France, I have been working for 10 years with lasers, so that I now cannot imagine everyday work in my practice without them. From my point of view, it is a real all-rounder that offers both me and my patients many treatment advantages: Quite apart from the time savings, what impresses me about dental lasers is the usually scar-free wound healing and greater bacterial reduction, which, in turn, mean less postoperative pain for my patients. In my experience, the use of lasers can significantly optimize treatment results and thus increase patient satisfaction.
High absorption due to blue wavelength
I had the pleasure of being a participant in the SIROLaser Blue customer trial organized by Dentsply Sirona and I have been working with it since summer 2015. This enables us to consistently offer optimum treatment to our patients.
SIROLaser Blue is the first dental laser worldwide that integrates several laser diodes for three wavelengths: In addition to an infrared (970 nm) and red (660 nm) diodes, it also has a blue (445 nm) diode. It can therefore be used in all areas of soft tissue treatment and for soft laser treatment.
The SIROLaser Blue is suitable for a total of more than 20 indications and at the same time is easy and convenient to operate. The performance of the blue diode, whose light energy is particularly well absorbed by hemoglobin- and pigment-containing cells and tissue, is especially impressive from my point of view.
The high energy input results in rapid coagulation while not penetrating too far into the tissue. This reduces the risk of inadvertent damage to deeper tissue layers. Especially in surgical applications, the use of the laser is therefore practically indispensable for me.
Precise and more conservative incisions
The very high absorption rate of the blue diode in hemoglobin results in minimal bleeding and thus cleaner and more conservative incisions. Due to the simultaneously lower absorption of the 445 nm diode in water, correspondingly less heat is generated in the adjacent tissue.
In addition, the blue wavelength makes it possible for the first time to perform incisions in non-contact mode. This not only avoids activation of the fiber tip but means that there is no need to remove tissue residues from the fibers during treatment.
The SIROLaser Blue is an all-rounder which, with its three wavelengths, is a truly versatile solution. The cut created by the blue laser light is extremely precise and enables a rapid, neat incision with only minimal bleeding. Especially for soft tissue treatment, I could not imagine life without it. It is not just me as the user, but also my patients who benefit from the laser.