Are you prone to getting mouth ulcers? There are a number of different contributing factors and presentations of mouth ulcers; and thankfully most are harmless and heal on their own. However, there are some that can appear very similar but are in fact far more serious. If your mouth ulcer isn’t healing, we recommend you visit us immediately to assess the possibility of mouth cancer. Any mouth ulcer that has been present for more than three weeks must be treated as serious until proven otherwise.
What is an ulcer?
A mouth ulcer, otherwise known as a canker sore or an aphthous ulcer, occurs when there is a break in the skin of the mouth (mucosal lining), exposing the underlying connective tissue. It may have a 'crater-like' appearance and is often red and painful, similar to a blister in the mouth.
Most people experience a single mouth ulcer but it is not uncommon to develop several ulcers at once. Mouth ulcers affect both men and women, although women and teenagers are more commonly affected. The causes of mouth ulcers can be extremely variable, and there are a number of triggers that can be responsible.
Aphthous ulcers are the most common type of mouth sore, and are generally the result of some kind of trauma and/or reduced immune response. These sores typically heal in a week or two, but they can recur throughout the person's lifetime. 'Major' aphthous ulcers are greater than 1 cm in diameter and take much longer to heal. Common mouth ulcer causes that we see include:
An injury by something sharp, (toothpick, braces, denture, appliance, sharp food, accidental bite, hard tooth brushing)
Trauma from acidic or hot foods (pineapple, strawberries, citrus, hot drinks).
Reduced immune response due to stress or lack of sleep.
Hormonal fluctuations, especially in women and adolescents.
Lack of essential vitamins, especially B-12, zinc, folate and iron.
What is the cause of an ulcer?
In Children
Viral mouth sores are more commonly seen in children. Herpes simplex virus, which causes small, painful ulcers on the lips, mouth and throat, is often accompanied by fever and swollen neck glands. Preschool children are also vulnerable to a viral infection that produces small blisters on the hands and feet, along with the mouth ulcers—also known as 'hand, foot and mouth disease'. These conditions can be very uncomfortable and painful enough to interfere with eating, but they usually are not serious. If the child is healthy and has normal immunity, the viral infection usually clears up in 1 to 2 weeks.
In Adults
Further testing may be required to identify a possible systemic cause when there is no obvious cause for an ulcer presenting. Miscellaneous mouth ulcers are associated with a number of underlying conditions including: blood abnormalities, medication side effects, skin conditions that produce ulcers on other areas of the body, intestinal disorders (like Crohn's disease and ulcerative colitis), and radiation treatments in the head and neck area.
Unlike the relatively benign examples mentioned above, oral cancers may initially show up as a mouth ulcer. Oral cancer can present itself in many ways: some people first become aware of an ulcer that won't heal: these lesions are usually a painless mouth ulcer, but it doesn't come and go the way other mouth ulcers do. Any mouth ulcer that has been present for more than three weeks must be treated as serious until proven otherwise. Similarly, if you have developed a red , white or mixed red and white patch, you must urgently seek a professional opinion.
What are the stats for oral cancer?
If you look at the statistics, about 50% of people with oral cancer die from their disease even after extensive surgery and radiotherapy. While small oral cancers that are detected early have a 80-90% cure rate, many oral cancer sufferers don't see an expert until it is at an advanced stage.
Oral cancer mainly used to be a disease of older people, contracted after a lifetime of smoking and drinking (the main causes). But things are changing and both oral and maxillofacial surgeons are seeing an increase in young people with mouth cancer. This could be related to the spread of the human papilloma virus (HPV) through sexual contact.
What should I do?
Too many young people with oral cancer don't go to their doctor or dentist soon enough. This is either because they haven't heard of oral cancer or they don't believe they can get it because they don't smoke. The fact that oral cancer is becoming a serious cancer among younger people who don't drink or smoke is not getting through to people. Remember: young, fit and healthy individuals can get oral cancer too.
That's why youhave to take the time to complete a thorough oral-facial assessment for any changes, lumps or bumps in the soft and hard tissue in the entire head and neck region. Because early detection is the key and oral health is more than just your teeth! If you have noticed a mouth sore that won’t heal, be sure to book in a consultation with your dentist.
Biofilms are a collective of one or more types of microorganisms that can grow on many different surfaces. Microorganisms that form biofilms include bacteria, fungi and protists.
One common example of a biofilm dental plaque, a slimy buildup of bacteria that forms on the surfaces of teeth. Pond scum is another example. Biofilms have been found growing on minerals and metals. They have been found underwater, underground and above the ground. They can grow on plant tissues and animal tissues, and on implanted medical devices such as catheters and pacemakers.
Role of oral biofilm in the aetiology of disease:
Oral biofilm is medically important because it has broad implications for maintaining not only oral health but also systemic health. It is estimated that biofilms account for over 80% of microbial infections in the body. Research has undoubtedly shown that biofilm-dependent infections, including oral diseases such as caries, and periodontal and endodontic disease, thus pose major public health and cost concerns globally.
Periodontal disease, in particular, is considered one of the most prevalent diseases worldwide, affecting up to 50% of the world’s adult population, according to FDI World Dental Federation. Previous research has established connections between periodontal disease and preterm births, low birthweight, diabetes, and risk factors associated with cardiovascular disease and stroke. Globally, periodontitis is responsible for an estimated US$54 billion per year in lost productivity and a major portion of the US$442 billion spent annually on oral disease, according to the European Federation of Periodontology.
Control of oral biofilm:
Owing to the vast implications of oral biofilm for dental and general health, its effective control represents a major challenge. There is no question that the formation and maturation of oral biofilm need to be tackled by dental professionals across all specialties in all countries worldwide.
“The backbone of any therapeutic and preventive approach is the disruption of the intra-oral biofilm. An example of technologies that have been successfully demonstrated to aid supra- and subgingival instrumentation are air polishing devices with low-abrasive powders that can disrupt the biofilm on all intra-oral surfaces, including mucous membranes and difficult-to-reach subgingival areas, without harming the hard tissue and the even more vulnerable soft tissue,” Beikler explained. “Their effects can be augmented by antimicrobial and immune- and microbiome-modulating strategies. Regarding the latter, probiotics offer an interesting and promising alternative to the use of unspecific antimicrobial agents like chlorhexidine or phenolic compounds. However, additional research, that is, appropriately designed and well-structured multicentre clinical trials, is critically needed to fully appraise their therapeutic effects,” he continued.
Another major challenge that needs to be taken into consideration in this respect is that trying to eliminate a specific pathogen using antimicrobial agents may disturb the sensitive microbial ecology and eventually induce microbial dysbiosis of the oral cavity.
Education on oral biofilm:
Until the early 1990s, dentists confined their treatment for combating oral plaque to removing calculus twice a year because there was only limited understanding of biofilm. Over the past decades, research on and improved knowledge about the parameters that determine the development of oral disease have spurred the development of new preventive strategies. For instance, piezoceramic instruments and low-abrasion powders have made professional biofilm management safer, minimally invasive and more comfortable for both the patient and the dental practitioner. Moreover, the launch and further development of AIRFLOW devices by EMS fundamentally changed biofilm management and eventually resulted in the development of Guided Biofilm Therapy, an innovative concept for contemporary prophylaxis.
As research and development of new technologies and therapies continues to progress, so too does knowledge in the dental professional community need to advance for effective integration of these developments into everyday practice for the well-being of the patient.
“As biofilms can be found on all oral surfaces, it is clear that all dental disciplines, ranging from dental hygienists to orthodontists, are highly affected by oral biofilm and its sequelae,” highlighted Beikler. “Unfortunately, prevention is sometimes still considered to be toothbrushing augmented by some kind of professional tooth cleaning. However, the whole oral cavity should be the therapeutic focus of a systematic preventive approach.”
For those people who have wisdom teeth, they usually erupt in early adulthood. Wisdom teeth may cause dental issues like overcrowding, especially if they’re impacted. However, many people have plenty of room for their wisdom teeth and they have no problems with them.
During this age frame, many people also get braces or just have them removed. People are often concerned that the eruption of their wisdom teeth will affect the progress they’ve made with braces.
Like previously stated, many people have their wisdom teeth come in with no problems. The teeth grow in straight and don’t affect the person’s bite. So overall, no, wisdom teeth do not cause significant overcrowding in the front of the mouth or severely disrupt any progress that was made with dental work like braces.
However, if they do not come in correctly or if a person’s jaw simply doesn’t have room for the new teeth, they can cause overcrowding among the back teeth.
It’s important to note that wisdom teeth are not the sole reason a person’s teeth begin to move. It’s been confirmed that people’s teeth move over time with or without the help of wisdom teeth. Additionally, when people have their braces removed, they may neglect to wear their retainers. Without the use of the retainer, a person’s teeth may begin to shift again.
While wisdom teeth may not necessarily cause a major issue with the dental progress that has been made with braces, there may still be reasons to have a wisdom tooth extraction. There are many wisdom tooth concerns that may call for tooth removal surgery, including: Crowding of back teeth, Infected gums, Bone defects, Root resorption, Dental diseases.
If a wisdom tooth becomes impacted or doesn’t erupt straight up, this can cause significant problems for the person. While some people may experience absolutely no problems with their wisdom teeth or get lucky enough to not have any of these extra molars at all, others may experience problems with them.
Fortunately, impacted tooth removal is a common procedure and can provide relief from any pain and discomfort caused by these teeth. In fact, wisdom teeth removal is more common than dental implant procedures, which about three million people have every year.
It’s important to remember that it’s perfectly normal for your teeth to move as you age. If your wisdom teeth are beginning to come in and are causing you pain and discomfort, your dentist may refer you to an experienced oral surgeon to discuss having them removed.
A bitter or bad taste in the mouth can be a normal reaction to eating pungent or sour foods. However, when the taste lasts for a long time or happens unexpectedly, it can be concerning.
Taste is a complex sense that can be affected by many factors, including poor dental hygiene, dry mouth, or pregnancy.
A persistent altered taste in the mouth is known medically as dysgeusia. This taste is described as unpleasant and can last for a long time until the underlying cause is treated.
People with dysgeusia may experience a constant taste that they often describe as one of the following:
bitter, metallic, rancid or foul and salty.
The taste can be distracting, and may even make it hard to taste other things while eating or drinking. A person may still have the taste even after brushing their teeth. They may also experience other symptoms depending on the cause.
Causes
Many of the causes of a bitter taste in the mouth are not serious. However, the symptoms can be irritating and may interfere with a person’s regular diet or their enjoyment of daily life.
The following conditions can cause a bitter taste in the mouth:
Dry mouth
A dry mouth, also known as xerostomia, occurs when the mouth does not produce enough saliva. Because saliva helps reduce the bacteria in the mouth, having less saliva means that more bacteria can survive.
People with xerostomia feel a sticky, dry feeling in their mouth. This could be caused by factors such as medications, pre-existing disorders, or tobacco use. A person can also get dry mouth if they have a stuffy nose because breathing through the mouth can dry it out.
People with a persistently dry mouth should talk to their doctor for a proper diagnosis.
Dental issues
Poor dental hygiene can also cause a bitter taste in the mouth. It may also cause an increase in cavities, infections, and gum disease or gingivitis.
Many common dental issues can be avoided by regularly brushing and flossing the teeth. Some people may also find that using a tongue scraper helps to clear up some symptoms.
Using an antibacterial mouthwash in between brushing may help keep foul-tasting bacteria to a minimum. A range of mouthwash is available for purchase online.
Pregnancy
A bitter or metallic taste in the mouth is a common complaint during the first trimester of pregnancy.
The hormones in the body fluctuate during pregnancy. This variation can affect the senses, which can cause specific cravings and make some foods or smells seem disgusting.
Many people who are pregnant also notice a metallic, bitter, or tinny taste in their mouths. This can be annoying, but it usually goes away later in the pregnancy or after giving birth.
Burning mouth syndrome
Burning mouth syndrome is a condition that causes a burning sensation in the mouth. The feeling can vary, but many describe it as similar to eating spicy peppers. Alongside, some people may also experience a bitter or rancid taste in their mouth.
The symptoms of burning mouth syndrome may appear sporadically, but it can also be chronic and last for a long time.
Some people with the syndrome may have difficulty eating or drinking, while others may find that this relieves their symptoms.
Menopause
Women going through menopause may also experience a bitter taste in their mouth. This could be due to lower levels of estrogen in the body, which can lead to a secondary condition, such as burning mouth syndrome. It may also be due to a persistently dry mouth.
GERD or acid reflux
Gastroesophageal reflux disease (GERD) or acid reflux may be the source of an unwanted bitter taste in the mouth.
These conditions occur when the muscle or sphincter at the top of the stomach becomes weak and allows acid or bile to rise up into the food pipe.
GERD tends to irritate the food pipe, causing a burning sensation in the chest or abdomen. It can also bring about a foul or bitter taste in the mouth.
Outlook
Experiencing a bitter taste in the mouth is fairly common, and it should not be an immediate reason to be concerned.
Most bitter tastes are treatable, and a person may be able to manage this symptom while a doctor diagnoses the cause.
Once the cause is found and treatment begins, the taste buds should return to normal, and the bitter taste in the mouth should disappear.
Impetigo, is a common and highly contagious skin infection that mainly affects infants and children. Impetigo usually appears as red sores on the face, especially around a child's nose and mouth, and on hands and feet. The sores burst and develop honey-colored crusts.
Treatment with antibiotics is generally recommended to help prevent the spread of impetigo to others. It's important to keep your child home from school or day care until he or she is no longer contagious — usually 24 hours after you begin antibiotic treatment.
You're exposed to the bacteria that cause impetigo when you come into contact with the sores of someone who's infected or with items they've touched — such as clothing, bed linen, towels and even toys.
Risk factors
Factors that increase the risk of impetigo include:
Age. Impetigo most commonly occurs in children ages 2 to 5.
Crowded conditions. Impetigo spreads easily in schools and child care settings.
Warm, humid weather. Impetigo infections are more common in summer.
Certain sports. Participation in sports that involve skin-to-skin contact, such as football or wrestling, increases your risk of developing impetigo.
Broken skin. The bacteria that cause impetigo often enter your skin through a small skin injury, insect bite or rash.
Adults and people with diabetes or a weakened immune system are more likely to develop ecthyma.
Complications
Impetigo typically isn't dangerous. And the sores in mild forms of the infection generally heal without scarring.
Rarely, complications of impetigo include:
Cellulitis. This potentially serious infection affects the tissues underlying your skin and eventually may spread to your lymph nodes and bloodstream. Untreated cellulitis can quickly become life-threatening.
Kidney problems. One of the types of bacteria that cause impetigo can also damage your kidneys.
Scarring. The ulcers associated with ecthyma can leave scars.
Prevention
Keeping skin clean is the best way to keep it healthy. It's important to wash cuts, scrapes, insect bites and other wounds right away.
To help prevent impetigo from spreading to others:
Gently wash the affected areas with mild soap and running water and then cover lightly with gauze.
Wash an infected person's clothes, linens and towels every day and don't share them with anyone else in your family.
Wear gloves when applying antibiotic ointment and wash your hands thoroughly afterward.
Cut an infected child's nails short to prevent damage from scratching.
Wash hands frequently.
Keep your child home until your doctor says he or she isn't contagious.
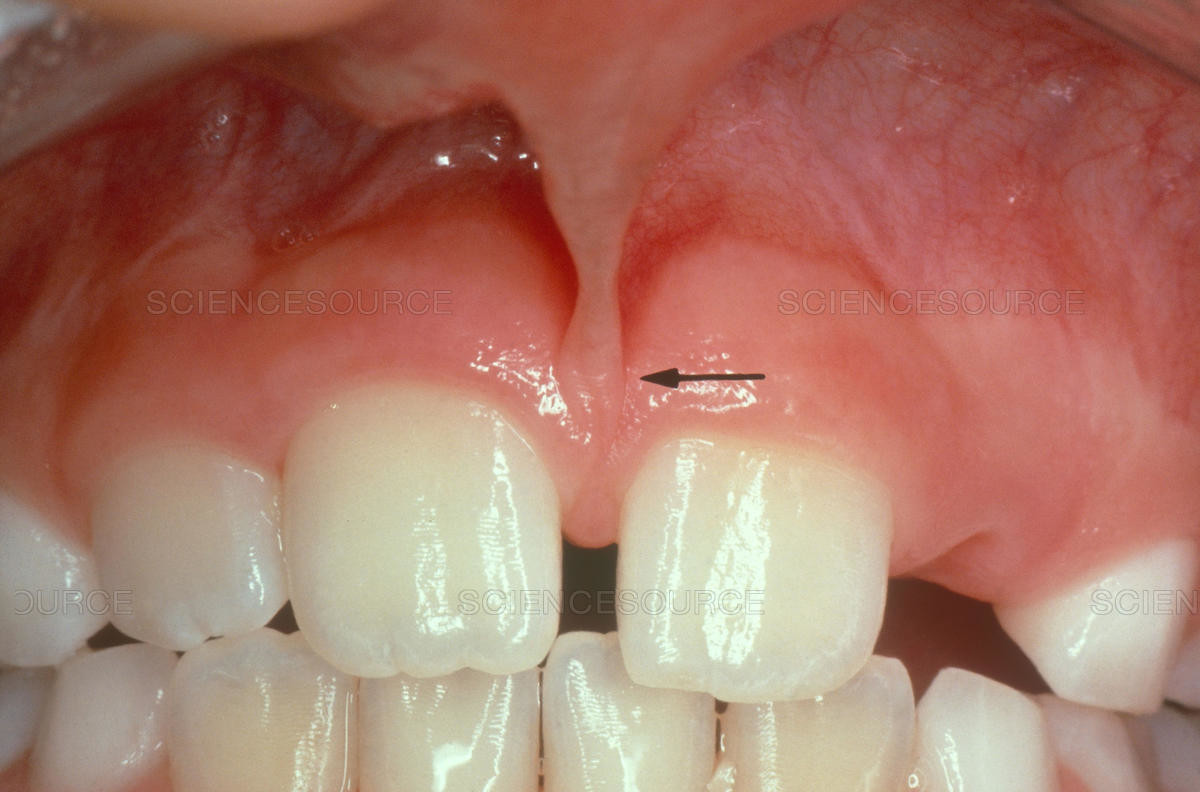
In our mouth, most people have two groups of tissue called frenums found in and around the gums and teeth. It is a piece of really soft tissue that appears as a thin line between the gums and lips. You can find it on the top and the bottom of your oral cavity. There’s also a frenum that extends along the bottom of the tongue and connects to the bottom of the mouth just behind the teeth. Different people have different frenums. It can vary in length and thickness.
Occasionally a frenum can get stretched or torn from kissing, eating, or wearing oral appliances like braces. Although this type of injury may bleed a lot, normally there’s no need for stitching or other serious medical procedure. Nevertheless, some dentists suggest treating a person with a cut frenum for indications of physical, cause this type of injury can often be a sign of abuse.
If your frenum tears constantly this may be painful and annoying so your dentist or oral surgeon may advise surgical removal. This type of operation is called a frenectomy. If you experience persistent problems with your frenulum mouth, teeth and gums may suffer severely if not treated properly.
Types Of Frenum
There are two basic types of frenums in your mouth:
Labial frenum – This type of frenum is placed in the front of your mouth between the upper lip and gum. His counterpart is positioned between the lower gum and the lower lip. If there is an issue with this type of frenum, it can change the way your teeth grow in and can influence your dental health. Particularly it can pull your gums away from a tooth revealing the root.
Lingual frenum – This type of frenum is located between the floor of your mouth and the base of your tongue. It comes in different sizes and sometimes it can limit the movement of your tongue. This means frenum is tight, and we call this condition: tongue-tie. If this happens, it can affect the way the tongue moves in your mouth. This problem is especially annoying for babies because it makes it hard for a baby to feed properly.
Historically, the absence of frenum was connected to various genetic and developmental conditions like Ehlers–Danlos syndrome.
Possible Problems With Frenum
The main purpose of a frenum is to give the lower and upper lip, as well as the tongue proper support and more stability in your mouth. If you suffer from an oversized frenum, it can lead to various problems that can affect your teeth, gums, and mouth.
Some of the conditions you may encounter if there’s an issue with a frenum include:
· frenum tear
· developmental malformations in your mouth
· trouble with swallowing
· speech difficulties if the tongue is tight
· disruption of the healthy growth of your upper two front teeth, which may cause a gap
· mouth breathing and snoring, due to deformities in jaw development created by abnormal frenum growth
· problems with nursing, due to lip-tie or tongue-tie in infants
· the gap formed between front teeth
· the difficulty of fully stretching your tongue
· receding of gum tissue away from the root of the teeth and revealing the tooth root.
Complications with the frenum may also happen after oral surgeries created by problems with operational techniques. An oral surgeon has to be extremely careful when cutting soft tissue in your mouth. Irregularities can cause the frenum to tear which may lead to constant problems with your teeth and gums.
What Is A Frenectomy?
A frenectomy is a procedure that removes your frenum tissue. Luckily, most people feel instant benefits after a successful frenectomy. This routine procedure normally takes a couple of minutes and is pretty simple to perform. Although it is still a surgery, the patient will be released in no time with minimal pain and discomfort in the following days. When performing a frenulum surgery the surgeon numbs the area and creates an incision to free it from being so tight or sometimes he removes it completely.
Stitches are only required depending on the size and severity of the frenum tissue. Modern “surgery” technique uses laser surgery, making less tissue damage, and scarcer bleeding for improved healing time.
Frenectomy may be used as a preventative measure, especially with young children without permanent teeth. It is important to point out that frenectomy won’t make your already spaced teeth come together. That is why it is recommended to complete any orthodontic treatment before you get a frenectomy.
Tasting, swallowing, talking – none of this would be possible without your tongue. But how often do you think about this group of muscles or pay attention to it? The tongue can often act as a unique view point into a person’s overall health and wellbeing, and dentists are often the first to spot problems that tend to arise gradually. However, pain, swelling, and discoloration can start up out of nowhere and cause serious discomfort and make it hard to eat and drink. Our Cary dentist is sharing some common tongue problems, what they mean, and whether you should call your doctor or dentist.
What Is a Healthy Tongue?
Before we look at symptoms of a problem, let’s first look at what a healthy tongue is supposed to look like. The tongue is a group of muscles that is covered in mucosa, a moist pink tissue and papillae, which are the small bumps that are covered in taste buds. Each taste bud is a collection of cells that connect to nerves that send taste signals to the brain, and while the four types of taste are sweet, sour, bitter, and salty, those tastes can be detected at every part of the tongue.
The tongue itself is attached by additional mucosa and tough tissue. In the front of the mouth, the tongue is held by the frenum, and in the back, it’s attached into the hyoid bone.
Common Issues in the Mouth and Tongue
Now that you know what a healthy tongue is supposed to look like, when there’s something wrong, like pain or discoloration, you may be inclined to call your doctor or dentist immediately. We understand, especially when it’s hard to eat or talk, but if you’re not sure when to worry or when to wait it out, these are the common tongue problems that often go away with at-home care.
Geographic Tongue
If your tongue has raised, red spots that may have a whitish border around them, this is a harmless condition called geographic tongue. Often, the spots go away on their own and sometimes the bumps shift locations. It’s typically painless and harmless.
Black, “Hairy” Tongue
The papillae grow over time, and while brushing regularly and eating tends to wear the papillae down, sometimes they continue to grow a bit longer. When this happens, bacteria adheres to the papillae making the tongue look dark brown or black and the longer papillae look like hairs.
This isn’t common and not serious, and it’s most commonly found in people who don’t have good dental health habits. However, people with diabetes or who are taking antibiotics may experience this condition. It’s generally recommended to use a tongue scraper and brush regularly to clean the surface.
Canker Sores
These mouth ulcers are painful and unpleasant, but they are nothing to worry about. This common problem goes away on its own in around a week, and during this time they aren’t contagious. Research does point to stress being a cause, if you find yourself getting them regularly.
Tongue Problems That Require a Dentist or Doctor
If you experience signs of the following conditions, it may be a more serious problem that requires the attention of your family dentist or doctor.
Oral Thrush
Oral thrush is a yeast infection in the lining of the mouth that produces raise white patches on the mouth and tongue. Most commonly seen in babies, the elderly, and people who are immune compromised, this is a treatable condition that can go away in a few days with a mild antifungal medication.
Red or “Strawberry” Tongue
A red, strawberry tongue could be a sign of a folic acid deficiency, but in children, it could also be a sign of scarlet fever or Kawasaki disease. Both are serious and require medical attention immediately.
Bald Tongue
Atrophic glossitis is a condition in which the tongue loses bumps from the papillae, becoming smooth in texture. This is sometimes caused by a B vitamin deficiency or anemia.
Oral Cancer
Often starting as a white patch, growth, or ulcer on the tongue that grows steadily, oral cancer is a serious condition that is most often seen in people who smoke or drink alcohol in larger quantities.
(01/03/2021) by Sninski and Schmitt Family Dentistry
Around one in 700 babies are born with a cleft around the world.
In early pregnancy, different parts of a baby’s face develop separately and then join together. If some parts do not join properly, the baby is born with a cleft.
A cleft lip and/or palate is the most common craniofacial abnormality (a problem to do with the skull and face) which babies can be born with.
Cleft Lip
A cleft lip can range from a little notch in the coloured part of the lip to a complete separation of the upper lip which can extend up and into the nose. This can affect one side of the mouth (unilateral) or both sides (bilateral), and can be complete (meaning the cleft goes up into the nose) or incomplete.
A cleft lip can also affect the gum where the teeth come through. Again, this can range from a small notch to a complete separation of the gum into two parts.
Sometimes a baby with a cleft palate may have a small lower jaw (mandible) and a few babies with this combination may have difficulties with breathing. This condition may be identified as Pierre Robin Sequence.
No one knows exactly what causes a cleft. Research tells us it’s often caused by a combination of different genetic and environmental factors.
Genetics is all about things inherited from family members, like eye and hair colour. With a cleft, sometimes there is a clear family link, other times it just happens as a ‘one off’.
How is it treated?
Surgery is needed to close the gap left by the cleft. This will usually happen when the child is under a year old.
Every cleft is unique, just like every child, so the exact treatment pathway will vary. It may include further surgery to help with issues such as speech and growth of adult teeth. It may also include speech therapy, help with hearing, orthodontic work, etc.
Dr. Suzanne Sablan enjoys helping people transform their smiles so that they can feel confident and pleased about their appearance, in addition to enjoying the health benefits associated with beautiful, properly-aligned teeth.
Having trained extensively in modern dentistry, including studies in Advanced General Dentistry, Orthodontics and TMJ, Dr. Sablan is uniquely qualified to assess your existing teeth, gums and jaw and help you achieve the look you want.
When people come to Dr. Sablan with something they want to fix or improve about their teeth or gums, she listens and advises them on how they can best achieve the look they want. She combines her naturally aesthetic eye with skilled use of high-tech dental procedures to reach and exceed expectations.
Dr. Sablan is especially good with children and very knowledgeable about all aspects of children's dentistry. Her friendly and calm manner reassures children and she has great success in helping children of all ages keep their teeth healthy and get any treatment they need.
Dr. Sablan is a mother herself, and has years of experience in helping parents and children take care of their teeth.
With our extended Saturday hours, we have many families that come to the dentist as a group. Dr. Sablan recommends that you start including your child in trips to the dentist from an early age so that they will become comfortable with tooth care as a routine activity.
Saliva, produced by the salivary glands inside the cheeks, under the tongue and at the floor of the mouth, protects your teeth against bacteria, assists in the digestion of food, helps with swallowing and lubricates your mouth. There are a number of issues that can interfere with the production or drainage process, leading to a variety of unpleasant symptoms.
Common Salivary Gland Issues
Problems with your salivary glands can be caused by a number of issues.
Salivary Stones:
Also known as sialoliths, salivary stones are formed from a buildup of crystallized saliva deposits. These stones can block the flow of saliva, causing pain and swelling. If they are not cleared, the gland can become infected.
Bacterial Infections:
When the ducts that drain saliva into the mouth are blocked, a bacterial infection can form. This leads to a painful lump in the gland and a foul-taste as pun drains into the mouth. When not treated, a bacterial infection can cause severe pain and a high fever.
Viral Infections:
A viral infection elsewhere in the body such as the flu or mumps can cause swelling in the salivary glands, specially the parotid glands on the side of the face.
Viral infections including Epstein-Barr virus, cytomegalovirus, Coxsackievirus and HIV can also cause salivary glands to swell.
Cysts:
These pockets of fluids form when the flow of saliva is blocked, usually because of an injury, infection, tumor or stones. Cysts can interfere with your ability to eat or speak.
Tumors:
There are many types of tumors that can affect the salivary glands. The most common are pleomorphic adenomas and Warthin’s tumor. Both are benign (noncancerous) and form in the parotid glands.
Cancerous salivary gland tumors include:
Mucoepidermoid carcinoma
Adenocystic carcinoma
Adenocarcinoma
Low-grade polymorphous adenocarcinoma
Malignant mixed tumor
How Salivary Gland Problems Are Treated
The treatment of salivary gland issues depends on the cause.
Conditions that block the ducts can be treated with a warm compress or sucking on sour candies to help increase the flow of saliva. If this does not work, the stones may require manual removal or the surgical removal of the affected gland.
Tumors, both benign and malignant may be removed through surgery. Radiation and chemotherapy may be required to treat some cancerous tumors.
Medications will be prescribed to treat a bacterial infection.